Study: Black youth most likely to receive drug restraints for mental health
Findings revealed at the 2023 Pediatric Academic Societies Meeting
Reports and ProceedingsNon-Hispanic Black youth between the ages of 5 and 18 years old are more likely to undergo pharmacologic restraint during mental health crises than children of other races and ethnicities. The findings will be presented at the Pediatric Academic Societies (PAS) 2023 Meeting, held April 27-May 1 in Washington, D.C.
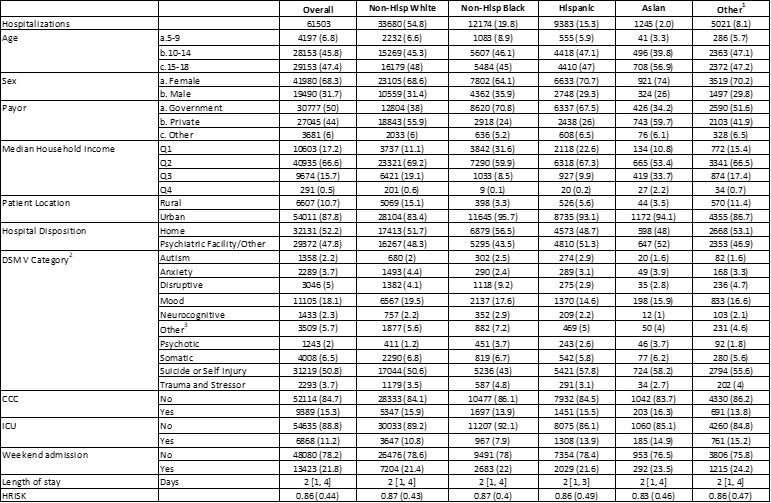
The study examined records of 61,503 children admitted to 41 non-psychiatric U.S. children’s hospitals between 2018 and 2022 due to mental health conditions such as autism, anxiety, psychotic disorders, self-injury or suicide, and trauma. Approximately 11.9% received pharmacologic restraint, a deliberate form of medication administered when there are acute safety concerns to staff and/or patient. The records were obtained from the Children’s Hospital Association’s Pediatric Health Information System database.
Among the 7,309 children who experienced pharmacologic restraint over the study period, 14.8% of children were Non-Hispanic Black, compared to 12.3% Hispanic, 11.6% Asian, 11.1% Non-Hispanic White, and 9.5% of other races and ethnicities.
Findings also showed that despite female hospitalizations (68.3%) outweighing those of males (31.7%), when evaluating for racial and ethnic differences in pharmacologic restraint by sex, Non-Hispanic Black male youth were more likely to undergo restraint. No differences were found among female sex and race/ethnicity.
“The study results reveal stark disparities in our hospitals’ care systems and point to evidence of interpersonal and structural racism in de-escalation of mental health crises,” said Ryan M. Wolf, M.D., pediatric hospital medicine fellow at Monroe Carell Jr. Children's Hospital at Vanderbilt and presenting author. “As America’s youth mental health crisis continues to grow, this data has drastic implications for evaluating pharmacologic restraint use during mental health crises.”
Researchers advocate that future studies should emphasize solutions to provide more equitable, preventive care for child and adolescent mental health patients that prioritizes their safety and minimizes disparities in health care facilities.
# # #
EDITOR:
Dr. Wolf will present “Racial/Ethnic Disparities in Pharmacologic Restraint Use for Children Hospitalized in Mental Health Crises” on Monday, May 1 at 8 a.m. ET.
Reporters interested in an interview with Dr. Wolf should contact Amber Fraley at amber.fraley@pasmeeting.org.
The PAS Meeting connects thousands of pediatricians and other health care providers worldwide. For more information about the PAS Meeting, please visit www.pas-meeting.org.
About the Pediatric Academic Societies Meeting
The Pediatric Academic Societies (PAS) Meeting is the premier North American scholarly child health meeting. The PAS Meeting connects thousands of pediatricians and other health care providers worldwide. The PAS Meeting is produced through a partnership of four pediatric organizations that are leaders in the advancement of pediatric research and child advocacy: American Pediatric Society, Society for Pediatric Research, Academic Pediatric Association and American Academy of Pediatrics. For more information, please visit www.pas-meeting.org. Follow us on Twitter @PASMeeting and like us on Facebook PASMeeting.
Abstract: Racial/Ethnic Disparities in Pharmacologic Restraint Use for Children Hospitalized in Mental Health Crises
Presenting Author: Ryan M. Wolf, MD
Organization
Monroe Carell Jr. Children's Hospital at Vanderbilt
Topic
Hospital Medicine: Clinical
Background
Children experiencing mental health crises are increasingly admitted to children’s hospitals awaiting inpatient psychiatric placement. For management of acute agitation, verbal de-escalation, pharmacologic restraint, and/or physical restraint are used. Little is known about racial/ethnic disparities of pharmacologic restraint use for hospitalized children.
Objective
Using a health equity lens, we examined the association between pharmacologic restraint use and race/ethnicity among children admitted for mental health conditions in acute care, non-psychiatric children’s hospitals.
Design/Methods
We performed a retrospective cohort study of children (5-18 years) admitted for a primary mental health condition from 2018-2022 at 41 US children's hospitals using the Pediatric Health Information System. Mental health conditions were defined using discharge diagnosis codes using a validated algorithm. Race/ethnicity data are reported by each acute agitation (Table 2 footnote). Race/ethnicity was considered as a sociopolitical construct and associations with pharmacologic restraint use were assessed using generalized linear mixed models with adjustment for clinical and demographic factors and then stratified by sex. To address potential misclassification, we performed a sensitivity analysis restricting the definition of pharmacological restraint to haloperidol, olanzapine, and ziprasidone.
Results
The cohort included 61503 hospitalizations (Table 1). Of those, 7309 (11.9%) had pharmacologic restraint use. Compared to Non-Hispanic Black children, those identifying as Non-Hispanic White, Asian, or other race/ethnicity were significantly less likely to receive pharmacologic restraints (range of adjusted odds ratios [aORs]: 0.68-0.82) (Table 2). When stratified by sex, observed racial/ethnic differences were magnified in males (aORs 0.49-0.68), and attenuated in females (aORs 0.83-0.93). In our sensitivity analysis, we observed significant and stronger negative associations with restraint use for all racial/ethnic groups (aORs 0.52- 0.64) as compared to Non-Hispanic Black youth.
Conclusion(s)
Non-Hispanic Black children, especially males, were significantly more likely to receive pharmacologic restraints than non-Hispanic White, Asian, and Hispanic children while hospitalized for mental health crises. Future work should focus on ways to promote more equitable care, such as implicit bias and verbal de-escalation training and standardized de-escalation protocols.
Tables and Images
{kind=link}
{kind=link}
No comments:
Post a Comment