It’s possible that I shall make an ass of myself. But in that case one can always get out of it with a little dialectic. I have, of course, so worded my proposition as to be right either way (K.Marx, Letter to F.Engels on the Indian Mutiny)
Monday, April 27, 2020
Most firms neglected to include pandemic in annual risk assessments despite warning signs, study shows
Public companies in the United States are required to file annual reports that, among other things, disclose the risk factors that might negatively affect the price of their stock.
The risk of a pandemic was known prior to the current health crisis, yet managers, in disclosing their companies' risk factors to shareholders in 2018, showed little foresight in terms of the impact and likelihood of a pandemic, according to new research from the University of Notre Dame.
In "Management Disclosure of Risk Factors and COVID-19," Bill McDonald and Timothy Loughran, finance professors at Notre Dame's Mendoza College of Business, examine all 10-K filings (annual reports filed with the Securities and Exchange Commission) from 2018, before the current pandemic, and find that less than 21 percent of the filings contain any pandemic-related terms.
"Pandemic risk was well known before today's crisis and we now know the impact for shareholders is significant and negative for the majority of companies," McDonald said. "Given management's presumably deep understanding of their businesses and general awareness that, for at least the past decade, pandemics have been identified as a significant global risk, the percentage of firms listing it among other low-probability events, like earthquakes, asteroids and volcanoes, should have been higher."
McDonald and Loughran applied their ongoing research, which utilizes textual analysis to gauge the tone of financial documents, to the coronavirus pandemic. And while they found many firms listed other low-probability events among potential risks, McDonald says legitimate warnings about pandemics dominated any real concerns about other types.
"Of course, hindsight makes things obvious," McDonald said, "but I think the risk of a pandemic was significant and, more importantly, it has the potential to cause more damage to most firms. A small portion of those firms, including Disney and Carnival Cruise Lines, acknowledged the risk."
Stock values have taken an enormous hit as a result of the pandemic, and McDonald says managers should have known better.
"Health organizations and reputable news sources had been emphasizing that a pandemic was a likely event," he said. "Informing shareholders of all potential risks associated with investing in a company is a critical part of the disclosure process. Perhaps companies need to go beyond standard templates in identifying unusual but relevant events that could impact the value of their firm."
How does alcohol kill this virus? With the onset of the COVID-19 pandemic, alcohol-based hand sanitizer became a much-sought item by hospitals and the general public alike for its ability to inactivate the coronavirus.
CIDD's Dr. Nita Bharti explains how the alcohol does this, and which concentrations are effective.
The ongoing COVID-19 outbreak has been a sort of Rorschach test. In addition to revealing deep strengths and ingenuity in the American community, it also has exposed some of America's deepest fears, xenophobic tendencies, and dysfunctions of leadership.
Those are among the conclusions of Hayagreeva "Huggy" Rao, the Atholl McBean Professor of Organizational Behavior and Human Resources at Stanford Graduate School of Business. Rao coauthored two studies in recent years that form the basis of his strong conclusions.
In one study, published in 2018, he studied the predictable rise of contamination rumors and ethnic violence that often follow an outbreak of an infectious disease. Rao says he and coauthor Sunasir Dutta of the University of Minnesota found that "exposure to discourse about contagious disease activates xenophobic tendencies in people. When you're exposed to this discourse, you're much more likely to believe rumors."
Rao's more recent study, done with colleagues Chelsea Galoni of the University of Iowa and Gregory Carpenter of Northwestern, looked at the underlying emotions triggered by contagious diseases.
"The conventional wisdom is that, if there is contamination, our response is one of disgust," Rao says. "But Chelsea, Greg, and I felt this was a somewhat incomplete account."
They concluded that perceived contamination actually triggers two emotions: disgust and fear. "There's a big difference between fear and disgust," he says. "With disgust, you know the cause is certain and that's why you shrink away. But with fear, the outcome is uncertain. That's why you're afraid. You don't quite know what's going to happen."
What does all of this show? "It lends credence to the idea that when you have a contagious disease, you become xenophobic and you perceive everyone else as a threat."
Is COVID-19 exacerbating cultural biases in ways you didn't expect, or is it playing out as your studies predicted?
If we know contagious disease can lead to xenophobia and loss of trust in strangers, what we need most is leadership. It's essential.
What kind of leadership?
First, we expect them to anticipate the unexpected. That doesn't mean they need to divine all of this by themselves, but we presume they have good people working for them and they listen to those people. However, leaders systematically underestimate the coordination difficulties going in. Some studies show that if you're in a leadership position, you're likely to underestimate coordination difficulties by at least 50%.
Second?
Leaders need to bear in mind that citizens are in a room called Fear, and they want to be taken to a room called Safe. Creating psychological safety is very important for leaders when you have contagious diseases. People expect to be assured that the community is committed to solving the problem. Even though the government may not be able to assure their continued existence, people need to be assured that everyone is doing their best.
So how is the U.S. leadership doing in that regard?
It's difficult for people to feel a sense of safety when they get conflicting messages, and when they see leaders display a blaming or scapegoating mentality. It's sort of weird that in the American narrative, exigencies, emergencies, and crises are frequently likened to war. Everything is a war. The war on drugs. The war on COVID. I'm a "wartime leader." Whatever. But if you really look at wartime leaders, they behave in a striking manner.
Striking in what way?
I think the best military leader America ever had was Matthew Ridgway. Ridgway was a brigadier general during World War II. He replaced Douglas MacArthur on the Korean operation. He'd never fought in Asia, never led a land battle. He had no idea about Korea. As soon as he took charge, he spent the first couple of days flying around Korea. He took the navigator's seat. They flew all over, noting rivers, lakes, mountains. Once he understood the geography and topography of Korea, he met regimental commanders and would ask them a series of questions to assess their leadership readiness. Often, his first questions had to do with geography. Where's the nearest river? How deep is it? If the commander wasn't able to answer, he was fired instantly because he was going to endanger their troops. That is wartime leadership.
Do you feel public officials typically help or hinder in terms of community cooperation?
Most of them want to do the right thing, including mayors and other community leaders. This morning I was reading about the school superintendent in the poorest county in Mississippi who is using his buses to deliver food to children who otherwise might starve. And he's doing it at some risk to himself. I find that extraordinary. That's leadership.
One key takeaway from one of your earlier studies was that the fear of contagion makes people irrational, as happened in the AIDS epidemic in San Francisco in the 1980s, when conservative groups focused on the morality of homosexuality rather than on managing the risks to public health. What's the most effective way to combat that sort of irrationality during a public health crisis?
The place to begin is to understand we're involved in a team sport. What's our job now? To help all of the people in the hospitals. How? By staying at home so we don't infect more people. In a team sport, everybody needs to commit.
What is it about the fear of contagion that makes otherwise rational people buy into unfounded rumors about those they consider to be outsiders?
One thing is that your own mortality becomes very salient. And then you add to that a fear of the unknown. You know you could die, but with no idea when or how. So there's all this uncertainty, and uncertainty is paralyzing. A good way to tame your fear—especially if leaders make it available—is to blame some other group for the origin of this. You have the Black Plague in the Middle Ages, and who got blamed? Jews got blamed. Take different contagious disease outbreaks, and usually a different group gets blamed every time. You can see this now in America.
How so?
We've had incidents of Chinese-Americans, Japanese-Americans, Korean-Americans who've been threatened, castigated, or criticized because the virus came out of Asia. That's the danger always with these contagious diseases. To put it simply, when we look at disasters, we often think the disaster is the problem. But what we need to understand is that disasters become catastrophes only when a society's cultural protections wither away or collapse. Our norms of civility, our norms of solidarity, begin to crumble when fear is coupled with disgust.
Is what's happening now just a continuation of the kind of xenophobia we've seen during past pandemics? Or is this something altogether different?
Xenophobia tendencies are always latent. They need opportunities to bubble up. You can think of COVID as one ramp by which this bubbling up happens. There are many, but that's one of them. It's not that COVID creates something out of nothing. The virus accentuates what's already there, lurking in the background, dormant. What COVID does is intensify it.
You sound pretty discouraged by what you've seen so far. But are there signs that give you hope?
I love what our students are doing, despite the fact that they're all afraid and thinking, "Am I gonna get a job? Am I gonna get an internship?" They're doing amazing things on campus, all on their own initiative. That gives me confidence. There are always tributaries of goodwill, solidarity, bringing out the best in people. My sincere hope is that this has been an education to the American people as to what government can and should do, and what venality can and cannot do.
In 2018 you concluded that a community's resilience hinges on two critical factors: How the disaster is framed by the community and its leaders, and how cooperative the community is in dealing with challenges. How prepared do you think the U.S. was for the coronavirus outbreak in terms of community cooperation?
We often think of preparedness as capability, but if you ask psychologists, they tell you preparedness is also motivation. It's a state of adaptive readiness. The short answer is that parts of the government, universities, public health people, and schools of medicine were certainly aware, and they were all highly concerned. The U.S. has some of the best contagious disease experts in the world. They're like Navy SEALs who specialize in vector-borne diseases. And yet we were not able to take advantage of their help. There was no understanding of all of this so it could translate into some sort of legislative strategy or set of executive priorities. It's been a confederacy-of-dunces kind of planning.
You've described charities and nonprofit organizations as critical factors in a society's resilience during a crisis such as this, because they help absorb the shock.
They are vital shock absorbers in any community. Take them away and you'll be in trouble. To my mind, this is another omission. I see all these budgets and outlays for businesses, and of course that's a useful thing to have, but what about nonprofits? Who's going to help them? They're the ones running the soup kitchens and doing the feeding and distribution. Without those shock absorbers, it's going to be very tragic.
You cite the work of public policy professor Robert Putnam of Harvard University, who compares social cooperation to the lubricant WD-40, which reduces friction. How do you rate our social cooperation during the coronavirus pandemic?
We need a lot more WD-40, sadly. In the end, be compassionate, be kind, and be generous. Period.
More information: Chelsea Galoni, et al. (2017), Pathogen Fear and the Familiar, in NA - Advances in Consumer Research Volume 45, https://www.acrwebsite.org/volumes/1023625
Coronavirus has emptied Venice of millions of tourists and its waters are no longer stirred by the thousands of boats, usually cross it
"The flora and fauna of the lagoon have not changed during lockdown. What has changed is our chance to see them," says zoologist Andrea Mangoni, plunging his camera into Venice's normally murky waters to observe life.
A crab tries to grab the intruding lens, jellyfish propel themselves along near the surface, schools of fish swim peacefully by, crustaceans cling to the city's famous jetties, and seaweed of every colour wafts gently on the current.
The coronavirus has emptied Venice of millions of tourists since the beginning of March and its waters are no longer stirred by the thousands of boats, taxis, vaporetti, and gondolas that usually cross it.
For Mangoni, this is an opportunity to rediscover the very diverse ecosystem that populates the Venice Lagoon. His film of a jellyfish swimming slowly though translucent canal water has gone viral on social media.
"Now we can see 50 or 60 centimetres, and sometimes even a metre from the surface. As a result, we can see animals that were literally hidden in the murky waters."
Mangoni says he has never seen such clear waters in the 20 years he has worked in Venice.
"The only difference is that some animals that before were relegated to bigger or wider canals in the lagoon, can now go as far as in the city centre since the traffic of gondolas, motorboats and smaller boats has ceased," he said.
Urban jelly fish
Marco Sigovini, researcher at the Institute of Marine Sciences of Venice (ISMAR-CNR), says he has seen marine species in the centre of the former city state for the first time.
With the boat traffic halted, marine species are being seen in the centre of the former city state for the first time
"Fauna and flora of Venice Lagoon are much more diversified and interesting than what one might think," he said.
"What decreased in the city is not only traffic with pollution produced by boats, but also the noise, which is another kind of pollution and disturbs many lagoon organisms."
Nevertheless, he is not surprised at how many jellyfish are being observed.
"Over the last 20-30 years jellyfish have increased in numbers generally. They come into the lagoon more and more frequently, particularly at certain times of year, perhaps carried by the current," he said.
"Normally, there's a lot of traffic so it's likely many of them are often killed."
Mangoni takes pictures and videos on his way to work and says life in Venice these days is "like being on a coral reef".
"The number of colours and lifeforms is extraordinary, which makes the lagoon unique," he said.
But Sigovini does not think much will change long-term for Venetian fauna.
"Most likely these few months of lockdown won't suffice to really change the quality of our ecosystem," he said.
A fish's eye view of today's catch from inside the canoe on a lake beside the River Purus during the low water season. Credit: Daniel Tregidgo
Poorer rural Amazonians are going hungry despite living in one of the most biodiverse areas on the planet—a new study reveals.
Massive seasonal floods mean many ribeirinhos, a marginalised social group who live alongside rivers in Brazil's Amazonian floodplain forests, struggle to catch enough fish to eat and can go hungry.
The Purus River, which flows towards the regional capital city of Manaus, undergoes one of the largest annual variations in water levels on the planet. When it floods, large areas of forest become submerged. River fish populations disperse making them much harder to catch.
The difficulty in catching fish during the floods might partially explain widespread malnutrition among vulnerable Amazonians, having serious lifelong health consequences, especially when affecting pregnant women and young children.
Policy makers and scientists had assumed that tropical areas containing very large forests contain enough food for the relatively sparse rural population.
Today, a team of scientists from Brazil and the UK are publishing the results of the first study linking food security for wildlife-dependent people in the Amazon with 'catch rates' - which is the amount of fish caught for each hour spent fishing.
Largely invisible to many policy makers and wider Brazilian society, the ribeirinhos, are some of the poorest people in Brazil, living in small communities dispersed over thousands of kilometres along Amazonian river systems. They often live far away from shops and lack electricity, refrigeration, or the ability to keep livestock. Therefore, ribeirinhos obtain a large proportion of their calories, macronutrients and micronutrients from catching fish.
Fishing for the world's largest freshwater scaled fish, pirarucu (Arapaima gigas), in a lake beside the River Purus. Credit: Daniel Tregidgo
During seasonal floods local people must spend around three times as long fishing compared to low water levels, using different techniques including more hooks, and fishing in different habitats—such as shallow flooded forests.
Despite their increased efforts fish catches fall by around half with catch rates reduced by 73 per cent.
This reduced food security during floods means families are forced to go without food for whole days, skip meals, or eat smaller portions.
Daniel Tregidgo, of the Federal University of Lavras in Brazil and Lancaster University in the UK is lead author on the study. He said: "The study highlights how the food security of marginalised rural communities living in a biologically rich area relies heavily on the stable supply of wildlife. Seasonal floods bring severe food insecurity among wildlife-reliant people by disrupting that supply despite being in an area of great natural wealth.
"This high prevalence of food insecurity seems paradoxical for Amazonian várzea forests which are biologically rich and have low human population densities but the population is highly dependent on this seasonally-transformed ecosystem.
"This study's findings indicates that we may be overlooking food instability in areas around the world where people are reliant on wildlife for food. This instability is potentially very common and dangerous for human health."
Researchers found that ribeirinhos also try to make up for their reduced fish catches by spending more time and effort hunting for bushmeat in the forests.
River Purus fisherman preparing the day's catch of tambaqui (Colossoma macropomum) and pirapitinga (Piaractus brachypomus) outside his house. Credit: Daniel Tregidgo
Paulo Pompeu from the Federal University of Lavras explains the potential implications of these findings across the Amazon: "Because the Amazon basin is experiencing a boom in construction of hydropower dams, such a major threat to fish stocks could lead to an increase in hunting pressure on land animals."
The findings that ribeirinhos both fish and hunt more when food security is reduced shows just how much they rely on wildlife.
The authors say that this evidence shows how effective management of river and forest wildlife populations is vital to ensure that remote rural communities can feed themselves in the high water season. Management of commercial fishing is particularly important, and the authors' previous research showed that fish stocks in the forest can be depleted by meeting the demand from large Amazonian cities, up to 1,000km away.
The study also found food insecurity hits the poorest hardest. Only the least-poor minority of ribeirinhos are able to protect themselves from seasonal food scarcity.
Researchers say the results show that the solution to food insecurity in the high water season is poverty alleviation for rural households. This raises important policy debates, particularly around welfare and fishing closed-season payments. They say that reliable provision of school meals in rural areas will also help support the diets of children in vulnerable households during times of low fish catches.
The researchers interviewed residents from 22 rural communities at least 13km apart from each other covering a distance along the river of 1,267km.
More information: Daniel Tregidgo et al, Tough fishing and severe seasonal food insecurity in Amazonian flooded forests, People and Nature (2020). DOI: 10.1002/pan3.10086
Before the United States can reopen safely, a new workforce at least 100,000 strong should be in place to trace the contacts of people diagnosed with COVID-19, according to a report from the Johns Hopkins Center for Health Security and other experts.
A long-used public health tool,contact tracingaims to break the chain of transmission of a contagious disease by identifying and alerting those who may have been exposed to it. Traditionally, a trained contact tracer will interview an individual diagnosed with the disease to determine all of their recent contacts, then reach out to those contacts to provide further information—which may include a recommendation to self-quarantine. In the past, this meticulous strategy has been used to help control Ebola, SARS, sexually transmitted infections, and tuberculosis, among other communicable diseases.
With the global outbreak of COVID-19, public health experts believe contact tracing will be a critical step for containing the virus, alongside social distancing and widespread testing. Many countries have already deployed extensive contact tracing, including New Zealand, Iceland, Taiwan, Singapore, and South Korea.
The United States, too, is gradually ramping up efforts—including a new hiring surge funded by the CDC, a Google/Apple tech partnership, and a statewide program in Massachusetts. In New York, Gov. Andrew Cuomo is working with Bloomberg Philanthropies to launch a massive contact tracing program that will include online training from the Johns Hopkins Bloomberg School of Public Health.
"In the absence of a vaccine, we think this is really the big public health tool we have to control transmission of COVID-19," says Crystal Watson, a lead author of the new report and assistant professor in the Bloomberg School. "We need to push hard for this."
The report acknowledges that a contact tracing effort of this magnitude—"and of this critical and historical importance for the functioning and reopening of society"—is without precedent. In an interview with the Hub, Watson offered more insight on the significance of this approach and the challenges ahead.
Is contact tracing on the scale the report suggests achievable in this country?
It's going to take a lot of work and some imagination and probably changing the rules in some ways to do things differently—but I do think it's achievable. We're seeing that other countries have implemented contact tracing and are able to contain the virus at a relatively low level in their communities.
We're also seeing parts of the U.S. start to put this in place, so that's encouraging, but it's not enough. We need to hire what we believe is up to 100,000 people or more to complete this work. So what we need first is funding and commitment from the federal government and Congress, to really scale this up in a way that's required. Our report suggests the need to dedicate approximately $3.6 billion for state and territorial health departments to make contact tracing wide-scale.
What are the likely outcomes if we try to reopen the country without robust contact tracing in place?
We don't know exactly how many people are still susceptible to COVID-19, but we're relatively confident that it's a very large percentage of our population. So if we reopen and we don't have the capacity to find each case, isolate them, then trace their contacts and put them in quarantine, this virus will start to circulate widely again in our communities, and we will see again a big surge of cases, a surge of hospitalizations, and a surge of deaths. If we don't reinforce these measures, things may get a lot worse.
As the report notes, privacy protections in the U.S. may prevent aspects of contact tracing we're seeing in other countries. What are the implications of that?
The U.S. won't be able to replicate a contact tracing effort like the one in South Korea, for example, which can use medical records, phone GPS records, credit card transactions, and closed-circuit TV.
We need to have conversations here about how to sufficiently protect privacy in this context. But there has to be a balance between personal privacy and getting health departments the information they need to act quickly. The Google and Apple partnership [to offer Bluetooth-enabled apps to track potential exposure to COVID-19] is promising, but it's unclear how public health officials will be able to use that information. I don't think we've struck that right balance yet with the technologies that are out there.
As unemployment skyrockets, to what extent can contact tracing create a new source of jobs?
This is a huge workforce that we need to engage. It may include many types of people: public health experts, retired health care workers, but also people outside the field. Contact tracing is an intensive activity, but it doesn't take a lot of time to train staff. We need people who are meticulous, who can make people comfortable and treat the task with sensitivity. Fluency in different languages is also a plus because we need to reach all communities.
So I think this is a great opportunity to put people to work who have either been laid off because of the pandemic, or who otherwise just want to be directly involved in the response.
As testing for the novel coronavirus continues to scale up, a new study finds that saliva samples are a "preferable" indicator for infection than the deep nasal swabs now widely used.
The study led by the Yale School of Public Health—and conducted at Yale New Haven Hospital with 44 inpatients and 98 health care workers—found thatsaliva samplestaken from just inside the mouth provided greater detection sensitivity and consistency throughout the course of an infection than the broadly recommended nasopharyngeal (NP) approach. The study also concluded that there was less variability in results with the self-sample collection ofsaliva.
"Taken together, our findings demonstrate that saliva is a viable and more sensitive alternative to nasopharyngeal swabs and could enable at-home self-administered sample collection for accurate large-scale SARS-CoV-2 testing," said first author Anne Wyllie, an associate research scientist at the Yale School of Public Health and a member of its Public Health Modeling Unit. She was joined by 49 other researchers at Yale on the study.
The researchers also reported that the saliva approach detected SARS-CoV-2 in two asymptomatic health care workers who had previously tested negative for the virus in a NP swab test. Saliva testing may be especially useful due to its accuracy in identifying mild SARS-CoV-2 infections that are not detected with other methods, the researchers said.
More sensitive and consistent detection is expected to be critical in helping to assess when individuals are able to safely return to work and when local economies can reopen during the current pandemic.
The study has not been subject to peer review. The research results are currently available on the pre-print server medRxiv. The researchers called for the "immediate validation" of the results. Nasopharyngeal testing is considered the gold standard for detecting many upper respiratory tract pathogens.
The study noted that saliva is an appealing alternative to NP swabs because:
Collecting saliva is minimally invasive to patients.
Saliva samples can be reliably self-administered.
Saliva has exhibited comparable sensitivity to nasopharyngeal swabs in detection of other respiratory pathogens.
The NP testing approach involves inserting a swab deep into the nostril and into the region of the pharynx. The swab is rotated to collect secretions and is then removed. The sample is then sent to a certified lab for analysis.
On April 13, the U.S. Food and Drug Administration gave emergency use authorization for a saliva-based test for COVID-19 developed by researchers at RUCDR Infinite Biologics, a biorepository backed by Rutgers University. The approved test must be conducted in a healthcare setting under supervision of a qualified professional.
"With further validation, widespread use of saliva sampling could be transformative for public health efforts," said Wyllie.
Saliva testing requires less resources, personal protective equipment, and personnel than nasopharyngeal swabbing, the researcher said.
"Once tests and laboratories are validated for using saliva, this could be rapidly implemented and immediately resolve many of the resource and safety issues with SARS-CoV-2 testing," said Nathan Grubaugh, an assistant professor at the Yale School of Public Health and one of the senior authors of the study.
Around the world, ventilators—a life-saving medical device that keeps air flowing into the lungs of a patient who is unable to breathe—are a scarce resource in hospitals and clinics where they're used to treat those infected with the COVID-19 virus.
The machines are expensive, complex, and they take a long time to make. They're also produced by only a handful of manufacturers, among them Medtronic, a medical equipmentcompanythat specializes in such devices. In response to the pandemic, the company has agreed to nearly double its production capacity, and recently offered to share its ventilator technology with other companies in order to accelerate production.
But if the antitrust laws regulating mergers and acquisitions by the Federal Trade Commission had been more stringent a few years ago, says economist John Kwoka, there wouldn't be such a limited number of suppliers dominating the ventilator market, which as a result has left us vulnerable to a shortage during a public health emergency.
"Everyone's concerned about how we got into this circumstance," says Kwoka, Neal F. Finnegan distinguished professor of economics at Northeastern. "And the answer is some of it was the result of planning too close to the margin, but some of it was the willful acts of companies seeking to prevent competition."
The Federal Trade Commission has shown a tendency over the past 20 years not to challenge mergers until the field of competition is smaller. The agency has also looked for benefits or reasons to approve mergers, says Kwoka, whereas in the old days, it took a more cautious approach, approving mergers only if they were clearly harmless or even beneficial.
One consequence of that has been a rapid consolidation in the medical equipment markets where a single company has ended up acquiring other relatively smaller companies that represented either competitive threats or overlapping possibilities.
"As a result of that process of consolidation, we have a much smaller number of very large companies with huge portfolios of products instead of a larger number of competitors in any single market," Kwoka says.
Similarly, the hospital industry has also undergone dramatic consolidation in the last 15 to 20 years—to the tune of close to 800 acquisitions, Kwoka says, many by hedge funds seeking to quickly maximize their bottom line.
This has left many communities, especially in rural areas, without a single hospital, and contributed to the steady decline and current shortage of beds across the country amid the pandemic.
"The Federal Trade Commission again has really not been active in challenging enough of these," says Kwoka. "They try to challenge some, to their credit, but with a tidal wave of mergers, it's been difficult for them to do anything other than take a look at the leading and largest examples."
The Medtronic case goes back to 2013 when, in an effort to supplement the national inventory, the U.S. Department of Health and Human Services contracted with Newport, a small startup supplier of ventilators. The department put out a series of specifications requiring a certain number of units and at one-third the price than the ones that were being produced by the major ventilator manufacturers in the country at the time, which included the Dutch firm Philips, and eventually a company called COVIDien (which was later acquired by Medtronic).
Newport had already produced some test models that met the specifications, says Kwoka. Nevertheless, the company was bought by COVIDien, which demanded a bigger contract from the government, and when the government only partially acquiesced, COVIDien withdrew from the contract and none of these new ventilators was produced.
"A number of observers at the time, and some government officials, thought—not surprisingly—that part of COVIDien's plan was simply to eliminate a lower cost potential competitor to its traditional ventilator operation," says Kwoka.
Consequently, he says, the effort to produce small, cheaper ventilators in large numbers to supplement the country's stockpile collapsed. The health and human services department eventually entered into a new contract with Philips, but years were wasted and that agreement still has yet to produce any ventilators.
"The long and short of it is that COVIDien wanted to keep a potential competitor—a cheaper substitute for its own equipment—off the market, and succeeded in doing so," Kwoka says.
The Federal Trade Commission, upon completing a cursory review of the COVIDien acquisition, deemed that it was not a competition issue, and therefore did not challenge it.
While it's "nearly impossible" to undo the existing acquisitions, Kwoka suggests that going forward, the Federal Trade Commission can be more vigilant about preventing similar mergers in the medical equipment area. And to address the shortage, he says that the major ventilator manufacturers can, as Medtronic has now agreed to do, disclose its designs to enable other companies to manufacture the devices.
Kwoka's forthcoming book, Controlling Mergers and Market Power: A Program for Reviving Antitrust in America, addresses the question of how to reform and revitalize antitrust policy, and merger control in particular, in the U.S, and provides a comprehensive roadmap for rebuilding the necessary policies, institutions, and practices of a vigorous merger control poli
Back in January, the "novel coronavirus" that had sprung up in the Chinese city of Wuhan was at most a distant worry for many people in the United States.
But SARS-CoV-2, the coronavirus that causes COVID-19, was already circulating in major U.S. cities, according to Alessandro Vespignani, Sternberg Family distinguished university professor, who directs Northeastern's Network Science Institute. And if we want to keep our communities safe going forward, we need to understand how we missed a virus that was right under our noses.
"We don't want to fall into this trap in the future," Vespignani says.
The discovery that the virus was already circulating in the U.S in January comes from a model that Vespignani and his colleagues have been using to study and predict the global spread of the virus. The model relies on human mobility and patterns of interaction, as well as the infection dynamics of the virus.
"The model allows us to go into what we call the invisible stage of the epidemic in the United States," Vespignani says. "We can simulate the arrival of infected people that were starting local transmission chains."
Research that the group released last month shows that the cordoning off of cities within China, as well as travel restrictions implemented by countries around the globe, came too late. The coronavirus was already out.
But how did we miss it? Why didn't we notice people getting sick?
"There was no large scale testing capacity in the US and Europe, and the guidelines were to test only people with a travel history," Vespignani says. "But when you get an infection from somebody who is already in the United States, you don't have a travel history."
It was January—the height of flu season, winter colds, and other respiratory illnesses. Even the few people with severe cases would not have drawn much attention without a history of recent travel to China.
"So what happened is that for a month and a half, the epidemic had gone unnoticed," Vespignani says. "Until you have a critical mass of cases. Then, at that point, you start to see the tip of the iceberg."
Cities that are hubs for international travel from China—New York, Seattle, San Francisco, Los Angeles—saw the earliest cases in the U.S. But similar chains of infection were beginning all over the world. By the time the U.S. was turning away or quarantining travelers from China, the coronavirus was already spreading through U.S. cities, and new cases were coming from Europe and other areas.
Given the amount of change our lives have undergone in the past few months, looking back to January may feel like ancient history. But understanding how and when these outbreaks started can help researchers make predictions down the line.
"If I have an epidemic that starts in early January, I can project a certain trajectory; if I have an epidemic that starts in early March, everything is shifted by two months," Vespignani says. "That's an infinite time for a disease like this one. So you really want to be as sharp as possible, down to the level of a single week, to have the right timeline now to inform what we will see in the next weeks or months."
And what the researchers are learning will also help us make smart decisions when the number of infections has dropped off and we begin to lift physical-distancing measures.
It wasn't enough to only test for the virus based on travel history to national or international hotspots, Vespignani says. If we don't have more extensive testing, and the ability to trace the contacts of each infected person, a second wave of infection could be building without our knowledge.
"We don't want to find ourselves in the same situation," Vespignani says. "We need to have all that so that we can make visible what, in principle, could be invisible."
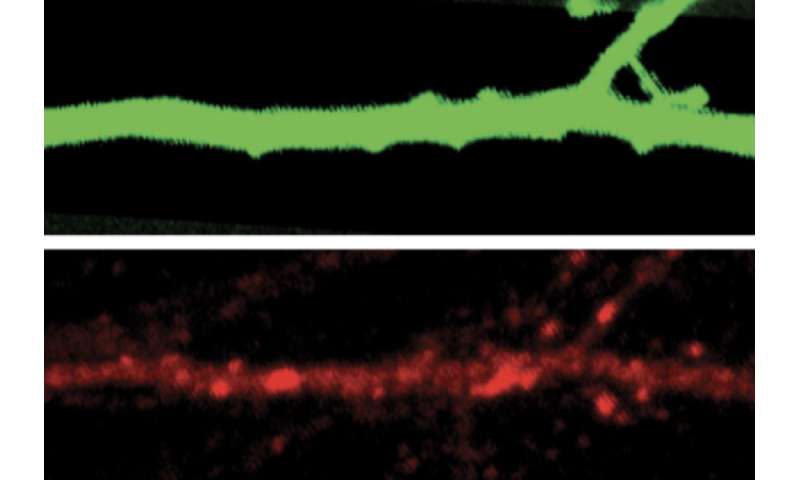
Lithium may treat behavior linked to autism gene by Peter Hess, Brandeis University
Altered responses: Neurons in mice missing a gene called SHANK3 do not respond well to changes in sensory input. Credit: Brandeis University
The mood-stabilizing drug lithium eases repetitive behaviors seen in mice missing SHANK3, an autism gene, according to a new study1.
The findings suggest lithium merits further study as a treatment for some people with autism, even though the drug has troublesome side effects, including tremors and impaired memory.
"Lithium is, of course, a rather difficult, non-ideal treatment," says lead investigator Gina Turrigiano, professor of vision science at Brandeis University in Waltham, Massachusetts. "It's really hard to get people on a lithium regimen that they can tolerate well." But understanding why lithium works may set the stage for better treatments, she says.
About 1 percent of people with autism have mutations in SHANK3. Deletion or mutation of the gene can also lead to Phelan-McDermid syndrome, which is characterized by intellectual disability, delayed speech and, often, autism.
Case studies of people with Phelan-McDermid syndrome also suggest that lithium eases behavior problems associated with the condition2.
Previous work has shown that SHANK3 helps stabilize neuronal circuits by adjusting excitatory and inhibitory signaling like a thermostat. This process, called homeostatic plasticity, allows neurons to respond to changes in sensory input.
The new study suggests the gene controls this thermostat by regulating how frequently neurons fire and how they adjust the electrical currents flowing through them. SHANK3 loss or mutation prevents neurons from adapting to changes in sensory input.
"What we've shown is there's this cellular mechanism, and loss of that mechanism is a direct result of a loss of SHANK3," Turrigiano says.
Firepower
The team first recorded electrical activity in rat neurons in which SHANK3 expression was partially disrupted. They artificially blocked the neurons' ability to fire. The mutant neurons' rate of firing did not return to its original range afterward as it did in control cells, the team found.
The neurons also responded with less electrical activity than controls did when the researchers blocked and then restarted electrical currents. This suggests the mutant neurons had lost their ability to adjust the current flowing through them.
Excitatory neurons in the cortex called pyramidal cells are most strongly affected. Lithium restored the cells' ability to adjust both their firing rates and how much current they carry.
To examine how neurons in mice lacking SHANK3 respond to changes in sensory input, the team implanted electrode arrays into the visual cortex of the mutant mice and controls and glued one eye shut in each mouse.
Over the following three or four days, the neurons in both groups of mice decreased how frequently they fired. But the decrease in the mutant mice was more gradual, suggesting that they take longer to adjust.
Neurons in the control mice returned to their typical firing rate two days after the rate had slowed to its lowest level, presumably because the mice's brains had adapted to the loss of vision in one eye. But in the mutant mice, the neurons never returned to their original firing rates, indicating that without the gene, their brains could not adapt.
The mutant mice also groom themselves excessively, a behavior that is thought to align with obsessive or repetitive behaviors in people. To the researchers' surprise, lithium stopped this behavior entirely. The work appeared in March in Neuron.
Treatment potential
The findings support the idea that lithium may help treat people with SHANK3 mutations, and perhaps those with other forms of autism as well, says Jean Martin Beaulieu, associate professor of psychiatry and neurosciences at the University of Toronto in Canada, who was not involved in the study.
However, he says, the study does not prove that the problems with homeostatic plasticity cause the repetitive behavior. Overgrooming is a complex behavior involving multiple brain areas, he says, whereas the study examined only the visual cortex.
It is also unclear whether lithium acts directly on SHANK3 or on some other target in the circuit, says Thomas Bourgeron, professor of genetics at the Institut Pasteur in Paris, France, who was not involved in the study.
Turrigiano says the loss of SHANK3 may be just the first step in a process that leads to neurons' inability to adapt to sensory input. Identifying which part of that process lithium corrects may point to new targets for treatment, she says.
Turrigiano's team is studying how SHANK3 helps balance excitatory and inhibitory activity of neurons, to better understand its role in maintaining homeostatic plasticity.
More information: Vedakumar Tatavarty et al. Autism-Associated Shank3 Is Essential for Homeostatic Compensation in Rodent V1, Neuron (2020). DOI: 10.1016/j.neuron.2020.02.033
Sylvie Serret et al. Lithium as a rescue therapy for regression and catatonia features in two SHANK3 patients with autism spectrum disorder: case reports, BMC Psychiatry (2015). DOI: 10.1186/s12888-015-0490-1