Janie McDermott and Annelies Goger
DEMAND FOR HEALTH CARE WORKERS IS HIGH, BUT JOB QUALITY IS OFTEN LOW
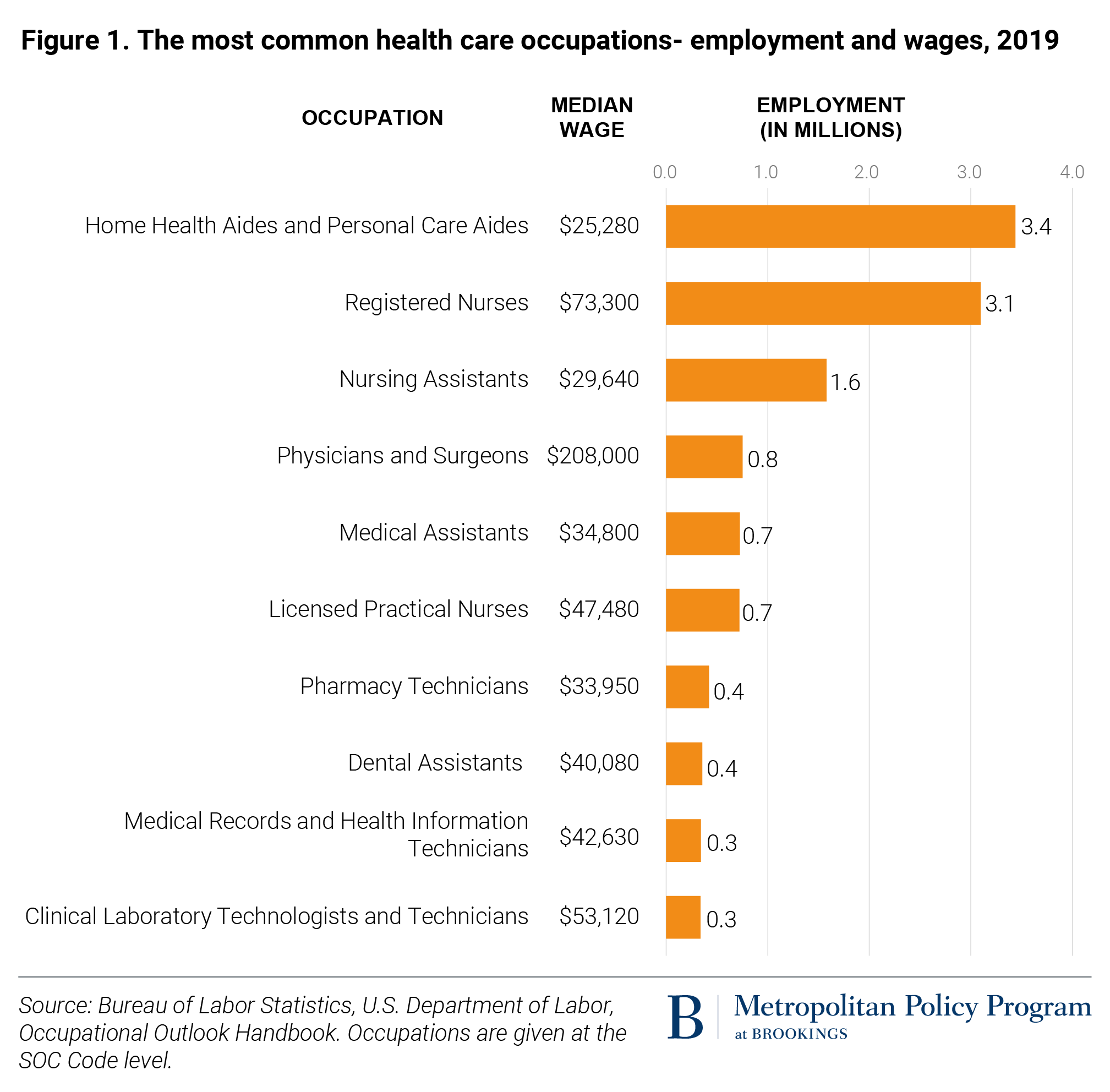
Following the passage of the Affordable Care Act in 2010, an influx of newly insured Americans increased overall demand for health care workers. The country’s aging population and high turnover in the field have also contributed to a need for more health care workers, particularly in long-term care settings.

Entry-level heath care workers can encounter a wide range of job-quality challenges. Low wages and part-time status keep roughly half of nursing assistants and home health aides living in or near poverty. Many low-wage health care workers are independent contractors rather than employees, making them ineligible for benefits such as paid sick leave and exempt from protections against harassment and discrimination. Approximately one in six direct-care workers in nursing homes and home health settings are uninsured. Low-wage health care workers often have unpredictable scheduling, and sometimes face penalties for not accepting last-minute changes.
These job-quality issues likely contribute to high turnover within these occupations, which is costly for employers. A 2020 survey found nursing assistants had a turnover rate of 27% per year (with a median income of $29,640), significantly higher than the turnover of 16% for registered nurses (with a median income of $73,300).
Low-wage health care jobs are highly segregated by race and gender, contributing to racial and gender equity problems in the broader labor market. As of 2019, 79% of workers in health services were women, and research suggests that health care work is undervalued precisely because it is associated with “women’s work.” Black workers make up nearly one-third of the direct-care workforce, which includes only lower-wage occupations. Because health care workers make up 12% of the entire U.S. labor force, occupational segregation in health care has a powerful effect on labor market dynamics.
PUBLIC INVESTMENTS IN HEALTH CARE TRAINING ARE CONCENTRATED IN LOW-WAGE OCCUPATIONS
WIOA adult and dislocated worker training programs largely direct participants into low-wage work (Figure 2). Annualized median earnings among health care training program participants exceeded $40,000 in only one occupation: registered nurses. Participants who completed nursing assistant training—the most common training among women—had annualized median earnings of just $20,002. Local workforce boards also place a very high share of female participants in health care training programs (Table 1), which perpetuates occupational segregation and, by extension, gender-based earnings disparities.

Black, Native American, and Latino or Hispanic women are particularly overrepresented in lower-wage health care training programs. Over one-third of Black women who participated in the WIOA Adult program were employed in health care occupations, and nine of the 10 most common training programs that Black women participated in were for health care jobs. Black women account for 36% of nursing assistant training participants, despite making up just 12% of those who exited the WIOA Adult program overall.
Local workforce development board investments in entry-level health care training are commonly justified because health care jobs are “in demand.” But they do little to address structural inequality and occupational segregation; arguably, they reinforce these issues by making it cheaper for employers filling low-wage jobs with high turnover to find a continual supply of labor, while also constraining the ability of workforce boards to invest in workers’ career mobility over the longer term.
LOW-WAGE HEALTH CARE WORKERS FACE BARRIERS TO ADVANCEMENT
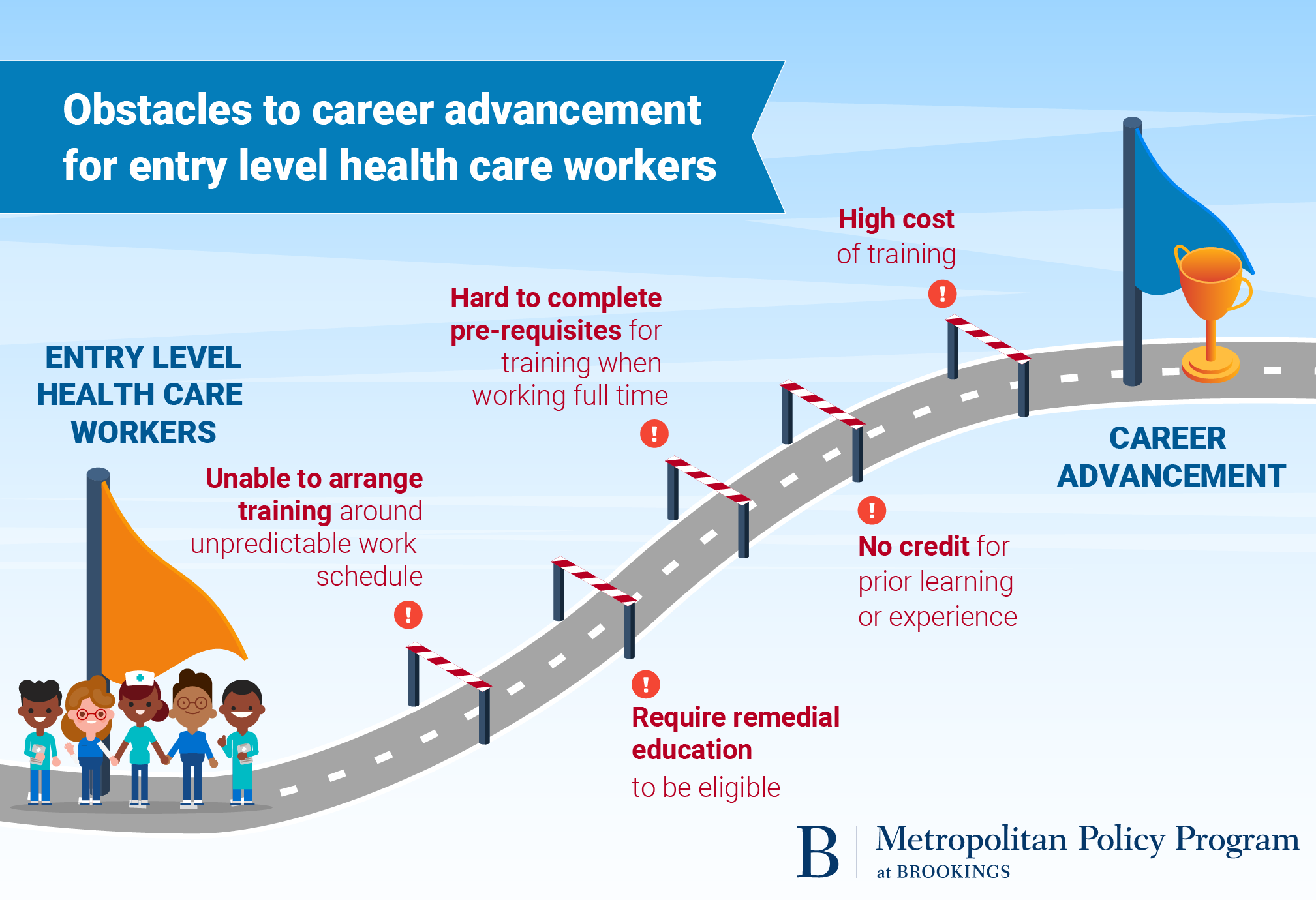
Low-wage health care employment doesn’t need to be a dead end. But to progress to higher-wage occupations, low-wage health care workers often face challenges such as entrance exams, high tuition and fees, and attending school while working full time. They also tend to have difficulty receiving credit for their prior learning and often need to start from scratch in order to progress within a career pathway.

Earn-and-learn models like apprenticeships have the potential to address some of these challenges, but accreditation and licensing bodies are often rigid in adapting the standards needed to pay apprentices. Health care apprenticeships also remain concentrated in many of these same lower-wage occupations. Nearly half (44%) of health care apprenticeships are the minimum length of one year, and the average hourly wage upon completion is $17.86.
Building a stronger health care workforce
Improving job quality for low-wage health care workers will likely require federal and state actions to improve standards and pay. These include:
Raising the minimum wage, raising reimbursement rates for Medicare and Medicaid, and creating wage boards.
Addressing volatility in scheduling by requiring more transparency, notice, and predictable pay.
Ensuring that frontline health care workers have consistent access to personal protective equipment, hazard pay, and paid sick leave for the duration of the pandemic.
Addressing structural inequality in the labor market will also require targeted efforts to support greater career mobility for the low-wage health care workforce, including the following strategies:
Change the dynamics of employer engagement: Publicly funded programs that offer worker training subsidies to health care employers can prioritize engagement with employers that show a demonstrated commitment to family-sustaining wages, desegregating the health care workforce, and career advancement.
Better coordination: Employers, workforce boards, training providers, and other partners should coordinate service strategies to offer a seamless career progression that is affordable and accessible to low-wage adults through funding, addressing service gaps, conducting outreach campaigns, and assigning clear roles.
Make it easier to obtain credit for prior learning: Establish articulation agreements and affordable prior learning assessment processes so workers can receive credit for their prior learning and work experience.
Employer investments:
Increase remediation and support: Increased investments in adult basic education, tutoring, and supportive services such as child care will help more health care workers advance.
Redirect resources to prioritize longer-term success and equity: Local workforce boards can focus on desegregating their training and placement activities in occupations that are already highly segregated by gender and race. They can also shift a higher share of their WIOA allocations to incumbent worker training (as opposed to entry-level training) or provide wraparound support to workers who are receiving tuition aid from other sources.
The COVID-19 pandemic has made clear that the health care industry and its workforce are essential to the U.S. economy, and will continue to be a valuable source of job growth in the economic recovery and beyond. However, the health care industry has a poor track record for advancing equity, and maintains extremely high levels of occupational segregation by race and gender. The country can either continue on the same path of using public funds to reproduce these structural inequalities and unsustainable business models, or take steps to ensure that all health care jobs offer decent working conditions, family-sustaining wages, and more opportunities for advancement
Wednesday, December 2, 2020
BROOKINGS INSTITUTE
Despite the onrush of corporate PR campaigns lauding the nation’s health care workers as the “heroes” of the COVID-19 pandemic, many of these workers report feeling underpaid and undervalued in their high-risk jobs. Entry-level roles in health care—such as home health aides or nursing assistants—provide critical patient care and are in very high demand nationwide. But workers in these positions must contend with very low wages, unstable hours, low access to benefits like health insurance, and limited career advancement options. Not coincidentally, these occupations are disproportionately filled by female, Black, and Latino or Hispanic workers.
Despite the onrush of corporate PR campaigns lauding the nation’s health care workers as the “heroes” of the COVID-19 pandemic, many of these workers report feeling underpaid and undervalued in their high-risk jobs. Entry-level roles in health care—such as home health aides or nursing assistants—provide critical patient care and are in very high demand nationwide. But workers in these positions must contend with very low wages, unstable hours, low access to benefits like health insurance, and limited career advancement options. Not coincidentally, these occupations are disproportionately filled by female, Black, and Latino or Hispanic workers.
DEMAND FOR HEALTH CARE WORKERS IS HIGH, BUT JOB QUALITY IS OFTEN LOW
Following the passage of the Affordable Care Act in 2010, an influx of newly insured Americans increased overall demand for health care workers. The country’s aging population and high turnover in the field have also contributed to a need for more health care workers, particularly in long-term care settings.
Entry-level heath care workers can encounter a wide range of job-quality challenges. Low wages and part-time status keep roughly half of nursing assistants and home health aides living in or near poverty. Many low-wage health care workers are independent contractors rather than employees, making them ineligible for benefits such as paid sick leave and exempt from protections against harassment and discrimination. Approximately one in six direct-care workers in nursing homes and home health settings are uninsured. Low-wage health care workers often have unpredictable scheduling, and sometimes face penalties for not accepting last-minute changes.
These job-quality issues likely contribute to high turnover within these occupations, which is costly for employers. A 2020 survey found nursing assistants had a turnover rate of 27% per year (with a median income of $29,640), significantly higher than the turnover of 16% for registered nurses (with a median income of $73,300).
Low-wage health care jobs are highly segregated by race and gender, contributing to racial and gender equity problems in the broader labor market. As of 2019, 79% of workers in health services were women, and research suggests that health care work is undervalued precisely because it is associated with “women’s work.” Black workers make up nearly one-third of the direct-care workforce, which includes only lower-wage occupations. Because health care workers make up 12% of the entire U.S. labor force, occupational segregation in health care has a powerful effect on labor market dynamics.
PUBLIC INVESTMENTS IN HEALTH CARE TRAINING ARE CONCENTRATED IN LOW-WAGE OCCUPATIONS
WIOA adult and dislocated worker training programs largely direct participants into low-wage work (Figure 2). Annualized median earnings among health care training program participants exceeded $40,000 in only one occupation: registered nurses. Participants who completed nursing assistant training—the most common training among women—had annualized median earnings of just $20,002. Local workforce boards also place a very high share of female participants in health care training programs (Table 1), which perpetuates occupational segregation and, by extension, gender-based earnings disparities.
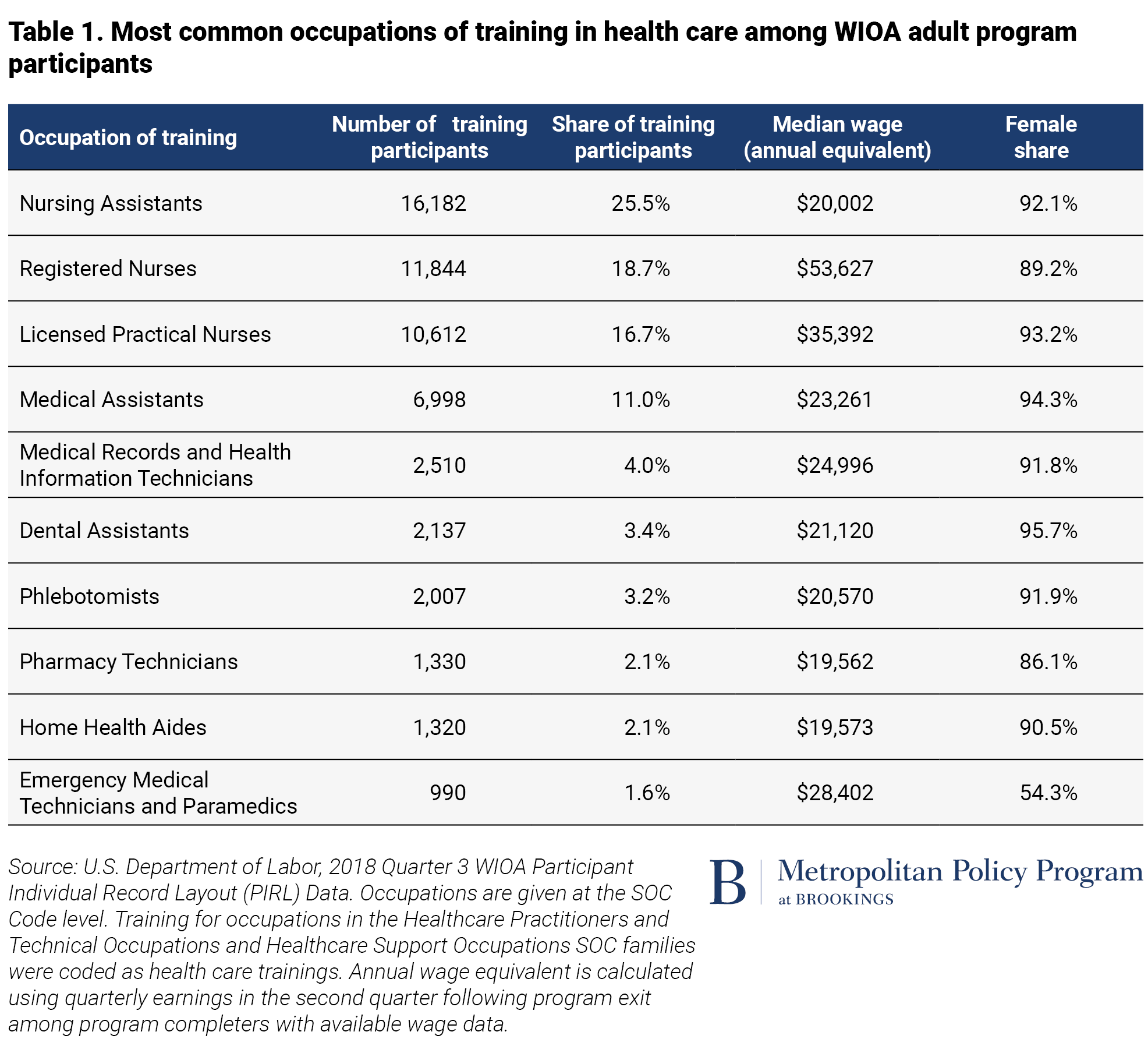
Black, Native American, and Latino or Hispanic women are particularly overrepresented in lower-wage health care training programs. Over one-third of Black women who participated in the WIOA Adult program were employed in health care occupations, and nine of the 10 most common training programs that Black women participated in were for health care jobs. Black women account for 36% of nursing assistant training participants, despite making up just 12% of those who exited the WIOA Adult program overall.
Local workforce development board investments in entry-level health care training are commonly justified because health care jobs are “in demand.” But they do little to address structural inequality and occupational segregation; arguably, they reinforce these issues by making it cheaper for employers filling low-wage jobs with high turnover to find a continual supply of labor, while also constraining the ability of workforce boards to invest in workers’ career mobility over the longer term.
LOW-WAGE HEALTH CARE WORKERS FACE BARRIERS TO ADVANCEMENT
Low-wage health care employment doesn’t need to be a dead end. But to progress to higher-wage occupations, low-wage health care workers often face challenges such as entrance exams, high tuition and fees, and attending school while working full time. They also tend to have difficulty receiving credit for their prior learning and often need to start from scratch in order to progress within a career pathway.
Earn-and-learn models like apprenticeships have the potential to address some of these challenges, but accreditation and licensing bodies are often rigid in adapting the standards needed to pay apprentices. Health care apprenticeships also remain concentrated in many of these same lower-wage occupations. Nearly half (44%) of health care apprenticeships are the minimum length of one year, and the average hourly wage upon completion is $17.86.
Building a stronger health care workforce
Improving job quality for low-wage health care workers will likely require federal and state actions to improve standards and pay. These include:
Raising the minimum wage, raising reimbursement rates for Medicare and Medicaid, and creating wage boards.
Addressing volatility in scheduling by requiring more transparency, notice, and predictable pay.
Ensuring that frontline health care workers have consistent access to personal protective equipment, hazard pay, and paid sick leave for the duration of the pandemic.
Addressing structural inequality in the labor market will also require targeted efforts to support greater career mobility for the low-wage health care workforce, including the following strategies:
Change the dynamics of employer engagement: Publicly funded programs that offer worker training subsidies to health care employers can prioritize engagement with employers that show a demonstrated commitment to family-sustaining wages, desegregating the health care workforce, and career advancement.
Better coordination: Employers, workforce boards, training providers, and other partners should coordinate service strategies to offer a seamless career progression that is affordable and accessible to low-wage adults through funding, addressing service gaps, conducting outreach campaigns, and assigning clear roles.
Make it easier to obtain credit for prior learning: Establish articulation agreements and affordable prior learning assessment processes so workers can receive credit for their prior learning and work experience.
Employer investments:
Employers should provide tuition assistance to frontline workers—particularly, pay-in-advance models that do not require low-wage workers to pay costs upfront.
Increase remediation and support: Increased investments in adult basic education, tutoring, and supportive services such as child care will help more health care workers advance.
Redirect resources to prioritize longer-term success and equity: Local workforce boards can focus on desegregating their training and placement activities in occupations that are already highly segregated by gender and race. They can also shift a higher share of their WIOA allocations to incumbent worker training (as opposed to entry-level training) or provide wraparound support to workers who are receiving tuition aid from other sources.
The COVID-19 pandemic has made clear that the health care industry and its workforce are essential to the U.S. economy, and will continue to be a valuable source of job growth in the economic recovery and beyond. However, the health care industry has a poor track record for advancing equity, and maintains extremely high levels of occupational segregation by race and gender. The country can either continue on the same path of using public funds to reproduce these structural inequalities and unsustainable business models, or take steps to ensure that all health care jobs offer decent working conditions, family-sustaining wages, and more opportunities for advancement


No comments:
Post a Comment