Iran Threatens to Attack Ships for Using Non-Iranian Routes Through Hormuz

Amidst a reported disagreement within Iran's leadership over whether to prioritize control of frozen bank accounts or control of the Strait of Hormuz, the Iranian senior military command center is signaling a strong preference for the latter - and a continued willingness to use force.
On Thursday, the Khatam al-Anbiya Central Headquarters - the Iranian equivalent of the Pentagon - threatened shipowners with attacks if they attempt to transit the Strait of Hormuz without approval. "Any failure to comply, deviation from the designated route, or disregard for the navigation protocols of the Islamic Republic of Iran in the Strait of Hormuz will be met with an immediate and forceful response from the armed forces," the headquarters staff said in a statement carried by state broadcaster IRIB.
There are three general routes through the strait at present: the northern, Iranian-controlled route past Qeshm; the preexisting Traffic Separation Scheme, which is believed to be mined; and a southern route along the Omani coastline, approved by the IMO and defended by the U.S. military. All are nominally free of charge during the 60-day period of negotiations between the U.S. and Iran, and Iran has agreed to make arrangements for unobstructed passage (contingent on the rest of the agreement being met). The Iranian military wants to ensure that all unobstructed passages happen under Iranian control, within Iranian waters, facilitating a post-MOU transition to a permanent Iranian control system for the waterway.
The U.S. government has offered to unfreeze more Iranian money held in overseas accounts, in effect exchanging funding for a more compliant Iranian approach to the strait, so far without success. Officials close to the diplomatic talks told the Wall Street Journal that U.S. negotiators have offered Iran access to some of its own blocked bank accounts - worth somewhere in the range of $6 billion, three times the amount of the 2016 cash payment approved by President Barack Obama - if Tehran agrees to give up control of Hormuz and set aside its long-term ambition to charge "service fees" for vessel transits.
The access to foreign funds would be a swift and much-needed windfall for the Iranian government, whether to provide for its own citizens in a severe economic downturn or to increase military spending and rebuild its missile and drone programs. It reflects a newly pragmatic approach by the administration: while still reportedly preparing for a military option, the White House appears open to financial solutions to the Strait of Hormuz problem - though at least in public, Iran is not taking the offer. Deputy Foreign Minister Kazem Gharibabadi said Thursday that the strait remains "under Iran's command."
The short-term payment might be far less than the long-term payoff if Iran could control Hormuz permanently (which some question on practical grounds). The Iranian government hopes to earn up to $40 billion every year in fee payments for crossings, according to the Wall Street Journal.
Oman Clarifies its Stance on Hormuz as Talks with Iran Widen

An uneasy calm appears to be prevailing in the Strait of Hormuz after the exchanges of fire between the United States and Iran, which followed the Iranian attack on the Singapore-flagged container ship Ever Lovely (IMO 9629110) on June 25. Both sides agreed on June 29 to stand down from these recent exchanges, to observe the ceasefire in a tighter manner, and also to resume technical discussions in Doha. In the background, and separate from the US-Iranian negotiations in Bürgenstock, bilateral discussions involving Iran and GCC states are taking place, with the GCC countries concerned that the talks in Switzerland will not deliver a lasting solution acceptable to all parties.
While a relative calm prevails, shipping is using both the Omani/IMO channel to the south, and a loosely-defined channel through Iranian waters to the north, with inbound and outbound shipping using the same channel, at a rate of about 60 transits a day. The volume of traffic is difficult to judge accurately, given that some ships are still traveling without switching on their AIS systems.
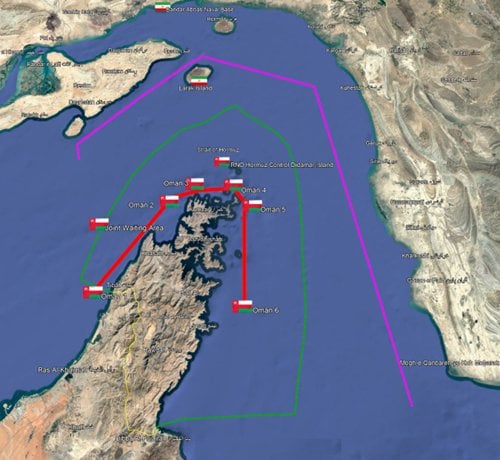
The Omani/IMO channel for exiting the Gulf (red), the inward and outward Iranian PGRA route (purple), and the extent of Omani territorial waters (green) (Google Earth, ©CJRC)
In the meantime, however, there had been some confusion about the Omani position regarding the Strait, attributable to poorly-sourced reporting and uncritical acceptance by the media of Iranian interpretations of the Omani position. Clarity was restored, however, when the Omani Foreign Minister, accompanying Sultan Haitham on a visit to France, gave an interview to Monte Carlo Doualiya, the French radio station broadcasting in Arabic. Sayyid Badr al Busaidi reiterated Oman’s position on Hormuz transits:
• Any bilateral understanding between Iran and Oman must fall within international law and UNCLOS.
• Oman is "not in favor of imposing transit fees. That is prohibited under international law, and we are committed to those rules."
• Oman is considering with Iran how environmental protection, navigational services, and emergency response can be improved in the Strait, drawing on the models in operation covering the Strait of Malacca and Singapore. Proposed future arrangements would be discussed and agreed upon with the international maritime community.
• Responsibility for mine clearance in the Strait rests with Iran, who should approach others for support if it was unable to fulfill its commitment to clearance of the Strait under the 14 Point MoU signed with the United States.
The statement makes it clear that while the scope and fee scale for services provided and charged for as Navigation Dues is under consideration in the discussions between Iran and Oman, charging tolls for passage, in effect creating a reconstruction fund, is not.
The statement also makes it clear that Oman will not unilaterally give permission for the European naval stabilization force to operate in the Strait. If the force is to be involved in mine clearance, then the permission of Iran needs to be sought.
Oman and Iran have already held a series of meetings to discuss management of the Strait, and a further such meeting occurred in Muscat on June 29. The meeting was chaired jointly by Oman's Sheikh Abdulaziz bin Abdullah Al Hinai and Iran's Deputy Foreign Minister Kazem Gharibabadi, who also led Iran’s delegation at the last similar such meeting in Muscat on May 24.

The Omani-Iranian Joint Committee meeting to discuss Strait of Hormuz navigation services, held in Muscat on June 29 (Omani MoFA)
Oman is keeping other GCC states closely informed on the progress of its talks with Iran over the Strait, in an effort to avoid misunderstandings, but also in an effort to build a new consensus. The Qatari Prime Minister Sheikh Mohammed bin Abdulrahman Al Thani visited Muscat to coordinate with the Omani Foreign Minister on June 23. The Omani Chief of Staff visited his opposite number in Bahrain also as part of this continuing dialogue on June 28.

The Omani Foreign Minister greets the Qatari Prime Minister in Muscat for a coordination meeting, June 23 (Omani MOFA)
At the same time, other GCC states are also conducting bilateral conversations with the Iranians. The Qataris are doing so as a consequence of holding a seat at the US-Iranian negotiations in Bürgenstock. The Saudi Foreign Minister Prince Faisal bin Farhan and his Iranian opposite number Abbas Araghchi held telephone discussions on June 24. The Times of Israel is reporting that these bilateral discussions with Iran outside the confines of the Bürgenstock talks will culminate in a regional conference involving Iran, to be held in Saudi Arabia, where the nations of the region will aim to establish a new political climate for living alongside each other.
Both Iran and the GCC have much to gain from a new security concord. If Pax Americana is not going to deliver peace in the region, then the nations of the region must establish a new modus vivendi among themselves, a development that would be equally welcome in the Gulf as in America, which would rather focus on problems elsewhere. The maritime community will breathe a sigh of relief if peace and stability can be established, at least some dividends to a highly disruptive war.
US Forces Still Poised in the Arabian Gulf Area

With an uneasy ceasefire having held now for some three days, which is something of a local record in recent times, there appears to be a determination shared by both Iran and the United States that there should be no further interruptions to the negotiation process, which has now switched to Doha and which is well behind schedule.
Nonetheless, the diplomatic and political climate remains tense, particularly among parties whose interests are not being directly represented by those conducting the actual negotiations in Qatar.
In Iran, a split in the ruling political elite, in which Paydari and IRGC hardliners seem to have the support of the hologram Supreme Leader Mojtaba Khamenei, has spilled into the open. There is open criticism of President Masoud Pezeshkian, Foreign Minister Abbas Araghchi, and the lead negotiator Mohammad Bagher Ghalibaf for being willing to conciliate, even though the Supreme National Security Council has given the go-ahead for negotiations to proceed. This has not stopped the hardliners, who contend that Iran has established an ascendant position following the war, from using their influence within media organizations to drip vitriol on their domestic political opponents and to press for the Islamic Republic to exploit its advantages by further developing its regional dominance. Moreover, the Iranian negotiating team has been accorded very little flexibility, which means that the talks in Qatar are in danger of collapse as soon as substantive issues come up for discussion. For the moment, while the week-long funeral of the late Supreme Leader proceeds, divisions may be put to one side, but may emerge once again in the coming days, along possibly with a first public appearance by Ali Khamenei’s elusive son Mojtaba.
There are also divisions on the other side of the Gulf. Some GCC states, notably Qatar and Oman, believe that the reality of Iran as it is today needs to be lived with. At the other end of the scale, the UAE sees the logical end-goal of Iranian ambitions as the dismemberment of the Gulf monarchies and the establishment of Iran as a regional super-power, displacing all outside influences and by implication the embedded positions of GCC countries in the global economy. In the middle, other regional countries profoundly distrust Iran, no longer have any doubts about its malign intentions, but want somehow to avoid any nastiness in the short-term. The lack of a unified position amongst Iran’s counter-parties is again a recipe for massive instability, which Commander Central Command was evidently seeking to redress when on July 2 a conference in Bahrain assembled military commanders from Bahrain, Egypt, Jordan, Kuwait, Lebanon, Oman, Qatar, Saudi Arabia, Syria, the United Arab Emirates, and Yemen to discuss the current regional security situation and coordinate protective measures particularly in regard to air defense.
If this was not enough, Israel regards the take-down of the Islamic regime in Iran as unfinished business, and the potential threat posed by an IRGC nuclear weapons program, the IRGC’s missiles and drones, and the evident ambition to rebuild the military capabilities of its regional proxies, all of which are regarded as a long-term threat to Israel’s survival. For the moment, Israel is happy to concentrate on achieving a potential solution to the instability on its northern border. But this diversion from tackling the long-term threat posed by Iran is likely to be only temporary if the US-Iranian negotiations do not produce a permanent solution.
In these circumstances, it is no surprise to see that CENTCOM is maintaining a high readiness posture.
Some forces have been withdrawn. Notably B-52 aircraft have been pulled back from RAF Fairford, and F-16 aircraft deployed to Saudi Arabia have returned to Aviano in Italy. F-15Es and F-35As from the 48th Fighter Wing are returning to RAF Lakenheath. A-10C Warthogs have staged home to Moody Air Force Base to Georgia through RAF Lakenheath. All these aircraft could return to the Middle East very quickly, save for the Warthogs which could only re-deploy at a more sedate pace as befits their tactical flight profile.
In the meantime, should conflict erupt once again, the element of the CENTCOM force that provides the forward screen and quick reaction force remains in place, providing Commander CENTCOM with the means to respond while reinforcements are brought back into theatre. This force in place consists principally of ground-based air defenses and assets afloat. CENTCOM for obvious reasons is not posting a daily order of battle, but two carrier strike groups remain in theatre, flag-shipped by USS Abraham Lincoln (CVN-72) and USS George H. W. Bush (CVN-77); in current circumstances, only one of these two CSGs is likely to be held forward, with the duties of the forward screen in the Gulf of Oman scaled back to reflect the lifting of the blockade on Iranian shipping and ports.
USS Boxer (LHD 4), USS Portland (LPD 27) and USS Comstock (LSD 45) with 11th Marine Expeditionary Unit are now in theatre, which suggests that the Boxer Amphibious Ready Group may now be taking over front line duties from USS Tripoli (LHA 7), USS San Diego (LPD-22) and USS New Orleans (LPD-18) with F-35Bs, tactical helicopters and the 31st Marine Expeditionary Unit embarked.
A key component of the continuing CENTCOM readiness posture appears to the presence of Apache helicopters over the Strait of Hormuz, protecting and covering the movement of shipping through the Strait, particularly those moving through the southern channel who continue to use the Omani coastal route. Maintaining the free flow of commerce through the Strait of Hormuz is a key CENTCOM objective at present, and also maintenance of the capacity to respond instantaneously should there be any attempts to interdict traffic.
In summary, while US forces are being both withdrawn from the theatre and rotated within the theatre to give front-line units opportunities for rest, resupply, and recuperation, a forward posture is being maintained so that there can be an immediate response to any Iranian breaches of the ceasefire, in particular in the Strait of Hormuz.