FROM THE ARCHIVES
The Deadliest Virus Ever Known
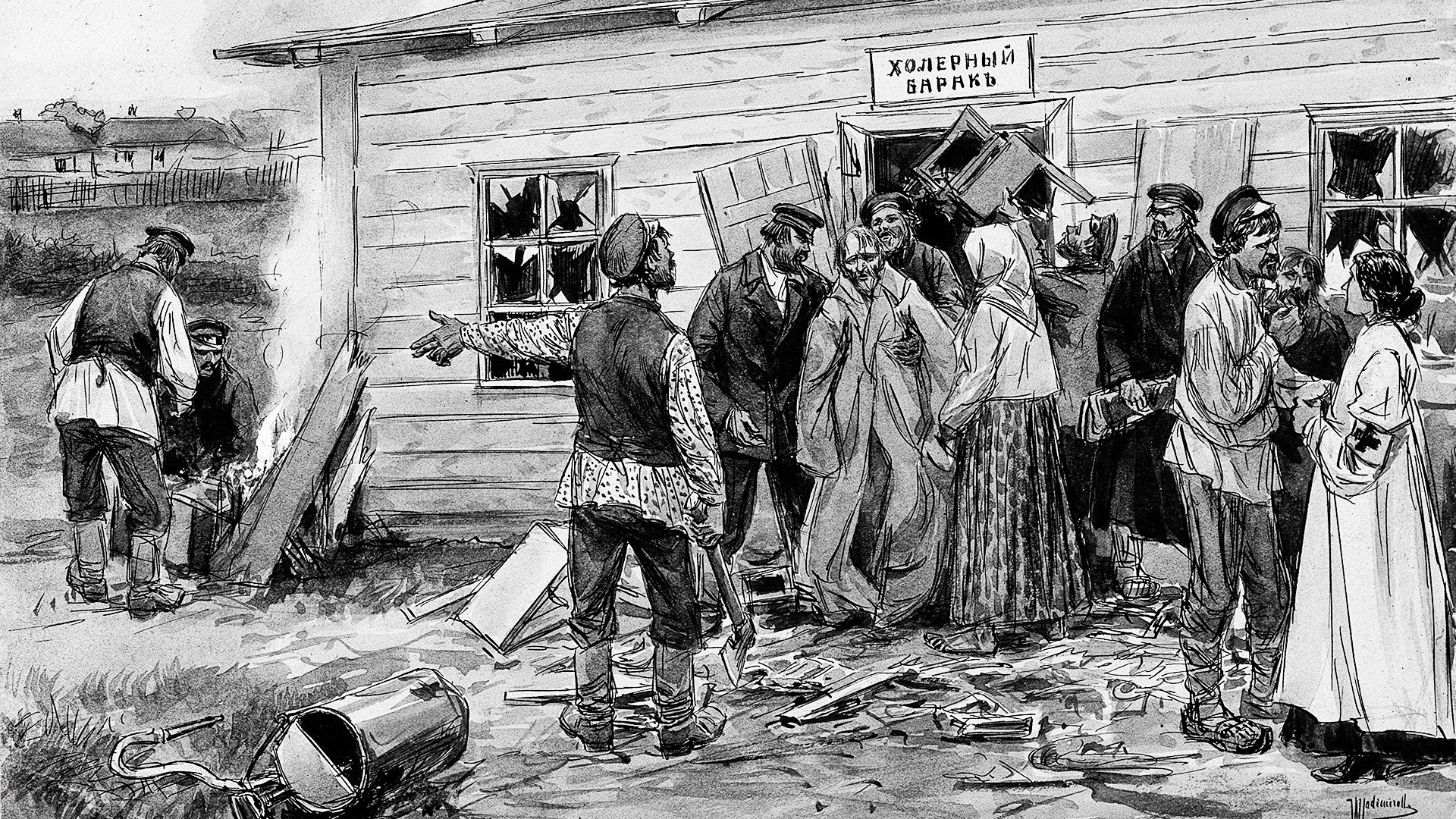
The Spanish-flu epidemic of 1918 reached virtually every country, killing so many people so quickly that some cities were forced to convert streetcars into hearses.
FOR SUCH A FORGOTTEN PANDEMIC PEOPLE SURE HAVE BEEN WRITING ABOUT IT FOR A LONG TIME
By Malcolm Gladwell September 22, 1997A Reporter at Large September 29, 1997 Issue
Photograph from Culver Pictures / Alamy
I—PERMAFROST
On September 24, 1918, three days after setting sail from Norway’s northern coast, the Forsete arrived in Longyearbyen, a tiny mining town on one of the Norwegian islands north of the Arctic Circle. It was the last ship of the year, before ice made the Arctic fjords impassable, and it carried among its passengers a number of fishermen and farmers going north for the winter to earn extra money in Longyearbyen’s coal mines. During the voyage, however, the ship had been hit with an outbreak of flu. Upon landing, many of the passengers had to be taken to the local hospital, and over the next two weeks seven of them died. They were buried side by side in the local cemetery, their graves marked by six white crosses and one headstone:
Ole Kristoffersen
February 1, 1896–October 1, 1918
Magnus Gabrielsen
May 10, 1890–October 2, 1918
Hans Hansen
September 14, 1891–October 3, 1918
Tormod Albrigtsen
February 2, 1899–October 3, 1918
Johan Bjerk
July 3, 1892–October 4, 1918
William Henry Richardsen
April 7, 1893–October 4, 1918
Kristian Hansen
March 10, 1890–October 7, 1918
The Longyearbyen cemetery is at the base of a steep hill, just beyond the town limits. If you look up from the cemetery, you can see the gray wooden skeleton of the coal mine that used to burrow into the side of the hill, and if you look to your left you can see the icy fringes of a glacier. Farther down the mountain are a shallow stream, a broad shale plain, and then, half a mile or so across the valley, Longyearbyen itself: a small cluster of red-roofed, brightly painted frame buildings. There are no trees, because Longyearbyen is many miles above the tree line, and from almost anywhere in the valley the cemetery is in plain view. Each grave site is slightly elevated and surrounded by rocks, and there are well-worn pathways among the rows of crosses. A chain-link fence rings the periphery. When I was there in late August, the ground had been warmed by the Arctic summer sun and was soft and spongy, carpeted with orange and red and white lichen. In the last row I found the miners’ graves—seven deaths separated by six days.
The New Yorker’s coronavirus news coverage and analysis are free for all readers.
It is possible to go to almost any cemetery in the world and find a similar cluster of graves from the fall of 1918. Between September and November of that year, as the First World War came to an end, an extraordinarily lethal strain of influenza swept the globe, killing between twenty million and forty million people. More Americans died of the flu over the next few months than were killed during the First World War, the Second World War, the Korean War, and the Vietnam War combined. The Spanish flu, as it came to be known, reached every continent and virtually every country on the map, going wherever ships sailed or cars or trucks or trains travelled, killing so many so quickly that some cities were forced to convert streetcars into hearses, and others buried their dead in mass graves, because they ran out of coffins. Of all those millions of graves, though, the seven in Longyearbyen stand apart. There, less than eight hundred miles from the North Pole, the ground beneath the lichen is hard-frozen permafrost. The bodies of the seven miners may well be intact, cryogenically preserved in the tundra, and, if so, the flu virus they caught on board the Forsete—the deadliest virus that the world has ever known—may still be down there with them.
At the beginning of next month, a scientific team led by the Canadian geographer Kirsty Duncan will fly to Longyearbyen and set up a workstation in the church graveyard. The team will map the site, and then scan it with ground-penetrating radar, passing what looks like a small black vacuum cleaner over the tundra to see how deep the bodies are buried. If the radar shows that they are below the active layer of the permafrost—that is, below the layer that thaws each summer—the team will return next fall with enough medical equipment and gear to outfit a small morgue. The site will be prepared with tarpaulins and duckboards. Pavement breakers—electric jackhammers—will be used to break up the tundra, and the chunks of earth will be scooped out with a shovel. As the excavation gets close to the coffins, the diggers will don biohazard spacesuits, and a dome or a tent will be erected over the operation.
To minimize the possibility of infection, the bodies will be left where they are, in their coffins, and autopsies will be performed in the ground. If the clothes on the corpses are frozen to the skin or tightly matted, someone on the team might run a hair dryer over the material to loosen it up—but only briefly. “If the bodies are thawed out and this material is taken out, it will melt, and then there is always the chance of the spread of microdroplets,” Peter Lewin, one of the team members, told me. Lewin is a pediatrician at Toronto’s Hospital for Sick Children who doubles as a medical archeologist, and he has earned international renown for his pioneering cat scans of Egyptian mummies. (He helped determine that Ramses V died of smallpox.) “Say you’re doing an autopsy”—he gestured to indicate a body spread out on the desk in front of him—“if it melts, there may be a mucousy, secondary blood product—some type of liquid exudation. The liquid seeping out of that material may suddenly, by mistake, be aerosolized and someone inhales it. You just don’t want to take any chances.”
From the ad-hoc morgue in the Longyearbyen cemetery, the samples will be flown to a BSL-4 facility—4 is the highest level of biological containment—either in England or at the United States Army’s infectious-disease research facility, at Fort Detrick, Maryland. There’s a small possibility that what scientists will find is a live virus—a virus that, once thawed, could be as deadly and infectious as it was in 1918. If they don’t, the hope is that they’ll at least be able to recover the virus’s genetic footprint—what scientists call RNA residue. Samples of the virus will then be sent to laboratories around the world. Its genetic code will be sequenced and compared with every major sample of the flu virus on file in the world’s virological centers.
This task has a certain urgency. Scientists know that global outbreaks of deadly influenza go back at least four hundred years, and that there have been two more since 1918—the Asian flu, of 1957, which killed seventy thousand Americans, and the Hong Kong flu, which killed thirty-three thousand during the winter of 1968-69. With luck, we’ll be able to anticipate the next Spanish flu before it does much damage. The problem is that we’re not really sure what to look for. No one kept a sample of the virus in 1918, because the flu virus wasn’t isolated until fifteen years later. And, because influenza mutates so rapidly, there’s almost nothing to be learned about the peculiarities of the 1918 virus from looking at the influenzas in circulation today. The only way to find out about the 1918 virus is to find the 1918 virus.
“We’ve designed core-biopsy-removal equipment to take core samples,” Peter Lewin said. “You drill into the body, because it’s solid. It’s a technique taken from forestry. You use what’s called a hole-saw tube.” He drew a diagram on the back of a file folder, outlining a long, hollow cylinder, with circular, screwlike grooves on its outside, a serrated edge on its tip, and a T-shaped handle at its other end. “It’s about nine inches long, about a quarter inch in diameter,” he went on, explaining that as the tube is twisted into a body it will collect a long cross-sectional sample of tissue. “We’ll probably take four core samples of the lung”—he pointed at the upper and lower chambers of his left and right lung—“one of the brain, one of the trachea, perhaps two of the bowel and liver.”
Lewin was raised in Egypt, where his father was a British military officer—two of Lewin’s schoolmates were Adnan Khashoggi and the future King Hussein—and he has the unflappable, genteel air of a nineteenth-century colonial explorer. He ticked off the details of the exhumation in Longyearbyen as if he were reciting a grocery list. “We’re doing some practice runs on frozen material—basically, on frozen pigs—to see if this thing works. We were initially going to use a drill. But the drill goes so fast that it heats the tissue up, and, of course, we don’t want that. So why not just slowly twist it in?” He rotated his hand. “They use hole saws on trees to get core samples of rings. They’re very useful. But no one has ever used them here. I mean”—he laughed—“how often do you do core samples of frozen bodies?”
II—THE SECOND WAVE
The first known case of Spanish flu was reported on March 4, 1918, at Camp Funston, in Kansas. By April, it had spread to most cities in America and had reached Europe, following the trail of the hundreds of thousands of American soldiers who crossed the Atlantic that spring for the closing offensives of the First World War. The spring wave was serious but not disastrous, and by midsummer it had subsided. A month or so later, however, the Spanish flu resurfaced. It was the same virus in the sense that if you’d got the flu in the spring you were resistant to it in the fall. But somehow over the summer it had mutated. Now it was a killer.
HOW DID THE SECOND WAVE GET TO NORTH AMERICA, IT WAS REACTIONARY ARMIES OF THE US, UK AND CANADA CALLED EXPEDITIONARY FORCES
THAT WERE TRYING INVADE RUSSIA VIA RONSTADT WITH THE WHITE ARMY IN TOW THEY FAILED AND WERE DEFEATED BY THE WORKERS AND SAILORS COUNCILS OF KRONSTADT.
The first case of the second wave was recorded on August 22nd, in Brest—a major port for incoming American troops. Within days, it appeared simultaneously in Boston and Freetown, Sierra Leone, carried in the former case by returning American soldiers and in the latter by H.M.S. Mantua, a British navy ship. The virus crossed Europe in a matter of weeks. It attacked Spain through Portugal, in the west, and across the Pyrenees, in the north, lingering long enough to be dubbed—erroneously, as it turned out—the Spanish flu. Scandinavia was infected by England; Italy was infected by France; and Sicily was infected by Italy. Allied soldiers coming to the aid of anti-Bolshevik forces during the Russian Revolution carried the flu to the White Sea area of northwestern Russia. European and American ships brought the flu to Iceland in mid-October, and American ships brought the flu to New Zealand at around the same time. In India, the virus came by sea and raced inland along the country’s railroad lines. As many as half of all those who died in the pandemic died within India’s borders. In America, an estimated six hundred and seventy-five thousand people died. In Philadelphia, seventy-six hundred people died within fourteen days. Putrefying bodies were stacked up three and four deep in the corridors of the city morgue, creating such a stench that the morgue was forced to throw open its doors for ventilation. In “America’s Forgotten Pandemic” (1976), a definitive history of the Spanish flu, the historian Alfred Crosby offered this description of the flu’s advance on Alaska:
On or about November 1 the virus reached the finest medium for its propagation in Nome and vicinity, the city’s Eskimo village. Few Eskimos escaped infection. In a single eight-day period 162 of them died. Some Eskimos, hounded by superstitious horror, fled from cabin to cabin, infecting increasing numbers with disease and panic. The temperature fell below freezing, and when rescuers broke into cabins from whose chimney came no sign of smoke, they found many, sometimes whole families, who had been too sick to renew their fires and who had frozen to death. When a number of Eskimos were rounded up from their separate cabins and placed in a single large building so they could be cared for efficiently, several of them responded to what they apparently perceived as incarceration in a death house by hanging themselves.
This was not the flu as we normally think of it. Typically, influenza infects the inner lining of the respiratory tract, damaging the air-filled cells of the lungs known as alveoli. Sometimes it brings on pneumonia. Usually it passes. This was much worse. “If you autopsied some of the worst cases, you’d find the lungs very red and very firm,” said Jeffery Taubenberger, a pathologist at the Armed Forces Institute of Pathology, in Washington, D.C. “The lungs are normally filled with air, so they are compressible. These would be very heavy and very dense. It’s the difference between a dry sponge and a wet sponge. A normal piece of lung would float in water because it was basically filled with air. These would sink. Microscopically, you would see that the alveoli would be filled with fluid, which made it impossible to breathe. These people were drowning. There was so much liquid in the air spaces of their lungs that patients would have bloody fluid coming out of their noses. When they died, it would often drench the bedsheets.”
Without sufficient oxygen, patients would suffer from cyanosis—a discoloration of the skin. “Two hours after admission they have the mahogany spots over the cheek bones,” a physician wrote at the time, describing the epidemic at Camp Devens, Massachusetts. “And in a few hours you can begin to see the cyanosis extended from the ears and spreading all over the face, until it is hard to distinguish the colored man from the white.” Nurses would triage incoming flu patients by looking at the color of their feet. Patients whose feet were black were considered as good as dead.
Something else was strange about the 1918 strain, and that was its choice of victim. Flu epidemics kill mostly at the demographic fringes—the very old, whose immune systems are the least robust, and the very young. Other adults do get sick, but they rarely die. In 1918, however, the usual pattern of mortality was reversed. The Longyearbyen seven, for example, were all between the ages of nineteen and twenty-eight, and that was by no means unusual. In the United States, men between twenty-five and twenty-nine died of the Spanish flu at several times the rate of men between seventy and seventy-four. This wasn’t just a deadly infectious disease. It was a deadly infectious disease with the singular and terrifying quality of being better at killing the young and healthy than the old and the infirm.
III—PROCESS OF ELIMINATION
Kirsty Duncan, the leader of the Longyearbyen expedition, is a medical geographer and climatologist by training, with dual appointments at the University of Windsor and the University of Toronto. We met in her parents’ house, a bungalow in the Toronto suburb of Etobicoke, she on one side of the family dining-room table, I on the other. Between us were five overstuffed black binders, filled with the results of four and a half years that Duncan had spent searching for frozen flu victims. In the kitchen behind us, Duncan’s mother prepared lunch. Whenever the phone rang, or the banging from the kitchen got too loud, or Duncan was coming to a critical part of her story, she dropped her voice almost to a whisper, so that I had to lean forward to hear what she was saying. She has large dark eyes and straight dark-brown hair that runs so far down her back that once when she got up her hair got caught in the chair. She’s thirty, but she looks much younger. When I first walked up to the house, I approached a woman watering the flowers and said, “Professor Duncan?” The woman replied, “Oh no. I’m her mother. Kirsty’s inside.”
Duncan’s obsession with the Spanish flu began when she read Crosby’s book on the pandemic. “I was absolutely fascinated—horrified, more than anything—that we didn’t know what caused this disease,” she told me. “I said to my husband, ‘I’m going to find the cause of the Spanish flu.’ ” The logical place to start, it seemed to her at the time, was Alaska, so she wrote to the Alaska bureau of Vital Statistics and had it ship her records from 1918. “I went through thousands of death certificates, and I found all kinds of cases of Spanish flu. The problem was trying to decipher where the permafrost was.” In 1951, the Army had led a secret expedition to a grave site near Marks Air Force Base, in Nome, to dig up 1918 corpses, but the mission—code-named Project George—failed for that very reason: the bodies weren’t in permafrost, and they had melted and decomposed. After Alaska, Duncan thought of Iceland. “But, of course, with all that geothermal energy it’s too warm,” she said. “Then I had a friend returning from Norway, and he mentioned permafrost, and I became excited, because I knew flu had been in Norway.”
Duncan’s focus was on the huge archipelago of islands, about six hundred miles north of Norway, that is known as Svalbard—and, in particular, on the town of Longyearbyen, a settlement of just over a thousand people which has served as Svalbard’s major port for the better part of the century. “I knew that people used to do coal mining in Svalbard,” she said. “I contacted the Norwegian Polar Institute. But they told me I had a really difficult task ahead of me. There are no medical records, because the hospital was bombed in the Second World War; no church records, because the first minister didn’t come out until the nineteen-twenties; and no government records, because Svalbard didn’t officially become part of Norway until 1925. They said there are these diaries, though, that the coal company kept.” Duncan called the coal company, which referred her to a schoolteacher in Longyearbyen. She called the schoolteacher. He found, in the 1918 entries, a record of the deaths of seven young miners from Spanish flu. “So now I knew that there were seven bodies, and that they were buried in the churchyard in Longyearbyen,” Duncan said. “I contacted the minister at the church. I said I wanted to know if the graves were marked. He said they were.”
The bodies of the seven miners are not, in all likelihood, perfectly preserved. Prolonged freezing desiccates soft tissue, so the best Duncan’s team can hope for is, essentially, natural mummies. “In a frozen state, the fluids in the body simply evaporate,” Michael Zimmerman, an anthropologist at the University of Pennsylvania and an expert on mummification, explained to me. “The process is called sublimation. It’s the change from the solid state to a gaseous state without going through a liquid state. If you put a tray of ice cubes in your freezer and go back two weeks later, they’re a lot smaller. That’s what we’re talking about.” Zimmerman estimated that the Longyearbyen seven, if they had been properly buried, would probably be down to about half their original weight, and maybe even less, so that their skin would be stretched tight over their bones, and every one of their ribs would be showing, as if they had been deprived of food for an extended period. “The eyes collapse, because there is a large fat pad behind the eye that’s mostly water, and when that dries the eye falls back into the socket,” he said. “Like everything else, the lips will tend to retract, so the teeth will become more prominent.” Nonetheless, Zimmerman thought that a full autopsy would still be possible. “I don’t see a problem,” he went on, “especially given that these bodies were buried only about eighty years ago. The tissues are probably still fairly flexible. They’re not like Egyptian mummies. Their tissues are like old leather, like an ancient book, and unless you’re careful they’ll crumble. Frozen bodies, since they don’t completely desiccate until they’ve been frozen for a thousand years, are still flexible. You can get big pieces out pretty easily.”
There is a catch, though. During the summer months, the top layer of the permafrost thaws. In Longyearbyen, that layer is between one and 1.2 metres deep. If the miners were buried in that layer—if the gravediggers in 1918 hadn’t gone to the trouble of blasting or pickaxing their way deep into the tundra—the bodies would be dust and bone by now. “I contacted the Norwegian authorities and asked what depth the bodies would have been buried, and they said, ‘Well, no one knows,’ ” Duncan went on. “Back then, that was no man’s land. But they assumed they would have followed the practice of the time, which was about two metres. The church minister believes they will be at two metres.”
This was more than simply a guess. In the permafrost, anything buried in the active layer will, over time, “float”—that is, be pushed up toward the surface by the continual expansion and contraction of the ground. For that reason, it’s relatively common in the hills around Longyearbyen to stumble across skeletons.
“If you go places where trappers are buried, you often see the coffin, open on the ground,” Kjell Mork, a Longyearbyen high-school teacher who serves as the town’s unofficial historian, told me. Mork is the man who gave the coal-company diaries to Duncan. He’s a dead ringer for the novelist Robertson Davies, and has in his house a polar-bear pelt that takes up almost an entire wall. “I see it all the time. Back in the sixteenth, seventeenth, and eighteenth centuries, the trapping teams had only two or three people, so they couldn’t take the effort to bury the bodies deep enough. Up at the northwest corner of the fjord, there used to be plenty of them. But now there’s a new ethic—to cover them up again. I think the polar bears were going there.” In the Longyearbyen churchyard, however, nothing has ever floated. Next to one of the crosses, just a few feet beyond the fence, I had seen a pile of fairly sizable white bones, including what looked like a human-size femur. But when I asked Mork about this he shook his head. “I think that’s just reindeer,” he said. “They come down the mountain to die.”
Duncan’s next big problem was to find out what had happened to the bodies before they were buried. The flu virus, after all, is notoriously unstable. It’s an RNA virus, as opposed to a DNA virus, and that means that instead of being composed of double strands of genetic code it has just one strand, and is much more vulnerable. The moment someone dies, enzymes are released that begin breaking down these nucleic acids and the genetic information they carry. A DNA virus, like herpes or hepatitis, could probably last in a body for a few days before being totally destroyed. But an RNA virus, like flu, would last between twelve and twenty-four hours at the most. The diaries kept by the manager of the coal company show that the bodies of the Longyearbyen seven were not buried until October 17th, ten days after the last of them died. What happened in those ten days? Did the bodies start to decompose before they were buried? Duncan was told that orderlies at the Longyearbyen hospital would have taken the bodies to an outdoor morgue while they waited for the graves to be dug. For there still to be RNA residue, the weather would have had to have been cold enough in those first two weeks of October to keep the RNA-dissolving enzymes at bay. She checked the weather records. The average temperature in early October was minus five degrees Celsius. Duncan had her bodies, and she knew where to find them.
IV—WAX MUSEUM
The Spanish-flu virus has been glimpsed just once, and that was in a scrap of lung tissue found two years ago in the National Tissue Repository, a division of the Armed Forces Institute of Pathology. The repository is in an annex of the Walter Reed Army Medical Center, in Maryland, just across the District of Columbia line, in a windowless corrugated-steel building behind a former elementary school. At the side are a parking lot and a loading dock, and there is an ill-kempt lawn out front. It looks like an industrial warehouse. Inside, there are three rooms, the largest of which is filled with rows of tall metal shelves, all stacked high with small brown cardboard boxes. Inside each of those boxes are pieces of human tissue about the size of a fingernail which have been preserved in formaldehyde and encased in a block of transparent paraffin wax. The repository holds more than two and a half million samples—some pressed between glass slides, some in boxes, some fully preserved organs—from autopsies on soldiers dating back to before the First World War. It’s the world’s largest library of death.
The supervisor of the repository is Al Riddick, a powerfully built black man in his mid-forties with a bald head, a gold chain, and glasses. When I toured the repository in late summer, Riddick took me to the back of the main room and pulled out a cardboard box from one of the shelves. Inside it were seventeen wax blocks, measuring roughly an inch by an inch by half an inch. “This is from a 1958 autopsy,” he said. He picked up one of the blocks, tilting it so that I could see a speckled, bright-orange sliver of tissue embedded in the wax. “That’s a brain block right there,” he said. Then he picked out another block, this one encasing a dark-reddish pockmarked rectangle that looked like a dried scab. “I would say that’s liver.”
Next, we walked into an adjacent room, where the Army keeps its collection of organs. On a lab bench was a plastic Ziploc bag with a heavy-looking, linen-wrapped object inside. “That’s a large surgical case,” Riddick said. “Could be a breast. Could be a lung. It’s big. Looks like a lung.” He picked it up in his hands, and began to knead the package delicately, as one might check a mango for ripeness. “No, there’s some bone in there.” He was as matter-of-fact as Peter Lewin had been in describing how to use a hole saw on a frozen corpse. I asked Riddick whether he was ever spooked, working in roomfuls of human parts. He shook his head. “Son,” he said. “I’m a Vietnam vet. It’s the people who move that bother me.”
In March of 1995, Jeffery Taubenberger, who heads the institute’s division of molecular pathology, called over to the repository to see whether it had any tissue samples from Spanish-flu victims. Taubenberger is not a “flu man,” meaning that he is not one of the small circle of scientists who have devoted their lives to influenza research. But he is one of the world’s experts in the arcane art of recovering genetic information from preserved tissue samples, and it occurred to him that he stood as good a chance of finding the Spanish flu as the scientists looking for frozen bodies. The archivists told Taubenberger that they had a hundred and twenty autopsy samples of flu victims. Some, though, were just microscopic slices of tissue between glass slides, and they didn’t give him enough material to work with. Taubenberger wanted wax blocks, which reduced his choices to seventy. Taubenberger and Ann Reid, a technician who worked with him on the project, randomly selected the medical records of thirty of those seventy cases. Of those, in turn, they rejected all the soldiers whose disease had not progressed rapidly, on the theory that those victims were less likely to have had the virus in their lungs when they died. That left them with seven cases. They were ready to begin.
Taubenberger and Reid started by taking lung samples from all seven and slicing off a microscopically thin sliver from the end of each block. “You take that slice and put it in a test tube and get rid of the wax,” Taubenberger explained. “And you take that tissue and spin it really fast, so it all goes to the bottom of the tube. You digest it in chemicals to chew up the membranes and the proteins, you go through a series of chemical purifications, and what you end up with is something highly enriched with the RNA.” Over an entire year, Taubenberger, Reid, and other members of their team worked to perfect a method of genetic analysis that could isolate the right material and stretch the tiny pieces of tissue they had as far as possible. Given the fragility of RNA, it was not an easy task. No one had ever recovered RNA from a sample so old. Early last year, they began testing the seven samples. One turned up positive.
Taubenberger is wiry and intense, with thick dark-brown hair and a patient, precise manner. He speaks in complete sentences and strings them together in complete paragraphs, until he has made even the most abstruse point crystal clear. I met him and Ann Reid in his office at the institute, a squat, five-story concrete bunker originally built as a nuclear shelter for President Eisenhower. The building has no windows, only a battered concrete doorway, and the walls inside are covered with tiles of a disorienting government-issue yellow. Taubenberger, Reid, and I sat in a circle, and the room was so small and cluttered that our feet were nearly touching. “He was a twenty-one-year-old army private,” Taubenberger said. “We know he died in South Carolina, at Fort Jackson. I believe he was from the state of New York. He had no prior medical history. He got sick at the height of the pandemic at Fort Jackson and had a fast downhill course. He presented with massive pneumonia and died six days later, on September 26th, at six-thirty in the morning. His autopsy was performed around noon.”
V—VIRAL SEX
One would think that, with the soldier’s sample in hand, many of the questions that surround the Spanish flu could be answered. In a certain sense, that’s true. Taubenberger and Reid have so far decoded about fifteen per cent of the genes in the soldier’s virus, and their work has made possible a few preliminary conclusions about the Spanish flu. It had already been hypothesized, for example, that the Spanish flu originated—at least, in part—with a bird, probably a wild duck. Waterfowl are what virologists call the “reservoir” for influenza. They carry most of the known subtypes of influenza—without apparent ill effect—and excrete them all in their feces, thereby spreading them through land and water to the rest of the animal kingdom. All animals that get the flu—horses, ferrets, seals, pigs, among others—and human beings probably get it originally from birds.
“At this time of the year in Canada, if you look at the wild ducks that are about to migrate south before the winter, around thirty per cent probably have the flu,” I was told by Robert Webster, a leading flu expert at St. Jude Children’s Research Hospital, in Memphis. “They’re popping it out in the water. If you sampled the lakes in Canada, you’d find all kinds of avian influenza.” At some point prior to the spring of 1918, then, a flu-carrying duck must have shed feces while flying over or nesting in some inhabited part of the world. If, in fact, the pandemic started in the place where the first case was reported—Camp Funston—the precipitating event was probably somewhere in or around Kansas.
That bird virus probably didn’t directly infect a human being, though, because human beings generally can’t catch flu directly from birds. Viruses are particular in that way. A virus infects and takes over a cell by latching onto what is called a receptor, but—as far as we know—there isn’t a receptor for avian flu in human beings. So how did the 1918 virus get from ducks to people? One possibility, according to Taubenberger’s analysis, is through pigs—one of the genes he studied looks like classic swine flu. This makes sense, because pigs, uniquely, have both human and avian flu receptors; they’re the perfect bridge between species. So perhaps the flu-contaminated duck feces dropped into a barnyard, whereupon a pig became infected while nosing in the dirt and passed the virus on to a farmer.
It’s not quite as simple as that, though, since another of the flu genes analyzed by Taubenberger looks very much as if it came from human flu. This wasn’t just bird flu passed on by a pig, in other words. This could well have been bird, pig, and human flu that somehow got mixed up together. The pig must have already been infected with one flu when it picked up the other: what it passed on to the farmer was a hybrid.
This is not as far-fetched as it sounds. A flu virus consists of eight gene segments that are so loosely bundled that they are like pieces of a jigsaw puzzle thrown together in a bag. If a pig got infected with avian and human flu simultaneously, the eight jigsaw pieces from the duck and the eight jigsaw pieces from the human being would be thrown together, and an entirely new puzzle could emerge.
Some scientists call this process of two viruses combining “viral sex,” which is an apt term, because, as in human reproduction, offspring split the genetic inheritance of mother and father. According to many influenza experts, this flukish interaction of separate species is probably how almost all the pandemic strains that periodically sweep the world first arise. The Hong Kong flu, for example, consisted of seven genes from an everyday human virus and one gene from a duck that combined inside a pig to create a nasty new hybrid. The Asian flu resulted from the same kind of reassortment.
Taubenberger couldn’t tell from his sample, though, what everyone really wants to know, which is what made the Spanish flu so devastating. It is possible to look at the flu strains that have proved deadly in domestic poultry and to explain their lethality almost entirely by pointing to an insertion mutation in one of the genes—a curious genetic glitch that allows the virus to attack almost any cell. One idea had been that the Spanish flu shared this same mutation. But Taubenberger showed that this wasn’t the case. The relevant segment of the soldier’s virus showed no such anomalies, and that meant that the secret of the Spanish flu’s lethality is probably somewhere else. Perhaps it lies in one of the genes that Taubenberger and Reid haven’t looked at yet. Or perhaps it’s not one mutation at all, but several, all combining in some subtle way.
“One thing to keep in mind is whether the virus that Taubenberger has is just a precursor,” Webster pointed out. “We’ve only got one virus so far. It might have been early in the pandemic’s evolution. Have we yet looked at the nasty bastard? We need more than one virus. One’s not enough.” With an earlier or later sample, Taubenberger could see what specific changes the virus made over the summer to become a killer. Just as good would be to find a strain from another part of the world which might have had a slightly different evolution, so that Taubenberger could eliminate the differences, and focus only on what the viruses had in common. But finding that second virus has proved difficult, since only the United States Army seems to have been so assiduous in hanging on to autopsy samples from the First World War. One famous pathology archive in Germany was destroyed in the Second World War. A handful of samples found in England have yet to turn up anything. Taubenberger has put out feelers to Spain and Italy, and found nothing. I asked him about Russia, since the Russians were also pioneers in medical record-keeping, but at that he and Reid burst out laughing. “There is an epidemiologist at the Centers for Disease Control who is Russian, and I spent some time talking to him about this when I was down there,” Taubenberger said. At this point, he dropped his voice an octave, imitating a thick Russian accent, and said, “October, 1918. Very bad time for Russia. Very bad time.”
This spring, Taubenberger met Duncan at a conference on the Spanish flu at the Centers for Disease Control, in Atlanta, and agreed to join her team. His lab will analyze whatever frozen samples she collects. The best hope for another copy of the Spanish flu, a second copy that will help make sense of the first, may well be lying in the permafrost of Longyearbyen.
VI—DRIFT AND SHIFT
Every year, early in the winter, the Food and Drug Administration hosts what some call the Flu Meeting, to insure that if the Spanish flu ever happened again we would not be unprepared. This year, the meeting took place on January 30th in the Versailles Ballroom of the Holiday Inn in Bethesda, Maryland, beginning at eight in the morning and ending at four. At the front of the auditorium, twenty or so medical experts sat behind a long table. Off to the side was a lectern, where throughout the day officials from the Centers for Disease Control and the World Health Organization gave presentations. The audience was large—well over a hundred—and included public-health officials from around the world, and vaccine manufacturers eager to get guidance from the government about what kinds of flu strains to put in the upcoming fall flu shot. Video cameras recorded the proceedings for those who couldn’t attend. Of the dozens of daylong conferences that the F.D.A. hosts every year, none are as important.
The first two speakers at this year’s meeting were from the surveillance section of the C.D.C.’s flu division—the eyes and ears of the flu world. Flu surveillance is critical because the flu virus comes in so many shapes and varieties. All flu viruses wear a kind of protective coat—an outer covering made up of two proteins known as hemagglutinin (h) and neuraminidase (n). That’s how you can tell a flu virus under a microscope. But there are at least fifteen varieties of h and nine varieties of n, and any one of the former can combine with any one of the latter to create a different virus family. For the past twenty years, the world has been dominated by two of these flu families—the descendants of the Hong Kong flu of 1968 and the Russian flu of 1977—and every year each of them spawns dozens of offspring: genetic variants that result as individual viruses spread from person to person and change to stay one step ahead of the human immune system. Whenever a new offspring emerges, virologists say the virus has “drifted.” At the same time, there is always the possibility that another avian strain will get mixed up with a human strain inside a pig and an entirely new family will emerge. If that were to happen, virologists would say the virus had “shifted.”
It’s this constant drifting and shifting that makes the flu so dangerous. If the flu stayed the same each year, you could be vaccinated against it the way you can be vaccinated against polio—for life. But, since the flu is always changing, the World Health Organization has had to set up a far-flung international surveillance network. Every day, in Moscow or Berlin or Iowa City or some distant Chinese province, doctors take nose and throat samples from flu sufferers, pack them in plastic vials, and send them to laboratories to be tested. The labs send isolates of the most interesting cases to the C.D.C. or to one of three other national labs working with W.H.O., in Tokyo, Melbourne, and London, for complete analysis, from which virus family trees are constructed.
Every known subtype of h and n has been identified and numbered, and every known strain has been labelled as well, with the city or the place-name where it was first isolated. If you got the flu last winter, for example, chances are you came down with h3n2 A/Wuhan/359/95; that is, a virus with No. 3 hemagglutinin, No. 2 neuraminidase, which was the three-hundred-and-fifty-ninth sample isolated from the Wuhan area of China in 1995. (The Wuhans were very big last year.) If you got the flu two years ago, on the other hand, chances are that you came down with something very similar to h3n2 A/Johannesburg/33/94.
At the Flu Meeting, the C.D.C. presented a road map of where the virus had travelled, and what forms it had taken during the previous year. It’s a fantastically detailed account, in which the flu virus comes across as a malevolent hitchhiker, stopping only to infect the locals before moving on. “February, there was a ship outbreak, the U.S.S. Arkansas, so severe that they brought the ship back into port,” Helen Regnery, the chief of the C.D.C.’s surveillance section, told the meeting as she explained the travels of the h3n2 strain throughout America last year. “The people on board the ship, almost one hundred per cent, were ill, with varying degrees of severity of illness.” On an overhead projector was a list of all the known offspring of the American h3n2 family, and Regnery pointed to another strain. “The Alaska/02 was an isolate in July. It is from a sporadic case and it has been sequenced, and will be on the sequencing tree. Hawaii in July had a nursing-home outbreak and increased activities. . . . Wisconsin, at a university, had an outbreak in September. New York/43 is from an H.I.V.-positive patient in November.” New Jersey followed, and then Indiana and Texas.
Regnery’s road map was intended to give the F.D.A. and vaccine makers a guide to the upcoming flu season. Vaccines consist, essentially, of a dose of virus that has been chemically deactivated, so that it will stimulate the immune system without causing disease. She was helping them to decide what virus strain to use. But if you want to inoculate a hundred million people you’ve got to grow enough virus to make a hundred million flu shots, and that takes time. Drug companies grow the virus in chicken eggs, injecting a microscopic droplet of flu virus into the air sac above the embryo and the yolk. There, in the nutrient-rich membrane of the sac, the virus grows until, after two or three days, the original droplet has become a tablespoonful. At that point, the tops of the eggs are lopped off and the virus is suctioned out. Mary Ritchey, an executive at Wyeth-Ayerst, one of the nation’s biggest flu-vaccine makers, told me that her company might use a hundred and fifty thousand eggs at a time, from which it might harvest two hundred and fifty gallons of pure virus. To supply the entire country with enough virus, vaccine makers have to do dozens of those batches, totalling millions of eggs. Then they have to purify the virus, test it, run it by the F.D.A., and then have it packaged, labelled, and sent to clinics around the country—all of which takes at least six months.
If the drug companies are going to have a flu shot ready for the fall flu season, then, they have to be told what strains to use by February or March. That means that the W.H.O.’s international surveillance teams have to guess what’s going to happen in the fall based on what they have seen the previous winter. There was a time, ten or twenty years ago, when this process was notoriously inexact: a flu shot might be prepared in the summer that offered only marginal protection against the flu strains that surfaced the following fall. With an improved surveillance system and more sophisticated genetic analysis, though, that has now changed. Every year, the C.D.C. gives itself a grade based on how closely the guesses made at the Flu Meeting correlate with the actual flu in the fall. For the last four years, those grades have been perfect.
If something like the Spanish flu ever came back, this is the system we are relying on to protect us. Right now, virtually all the flu in the human population is either h1n1 or h3n2, so the road map presented by the C.D.C. at the Flu Meeting was almost entirely an account of genetic drift within those two families. The minute that the C.D.C. or a W.H.O. laboratory received a flu that didn’t fall into the h1n1 or h3n2 families, it would sound the alarm. The surveillance system is also specifically focussed on those parts of the world where flu is prevalent and the interspecies movement that creates pandemic strains is more likely to occur. That means China, where there are as many ducks as people, and where pigs are often raised on farms in close proximity to wild and domestic poultry. China has been the source of the last two pandemics, and most observers think it likely that the next will be from there as well, possibly arising out of the marshy resting sites for ducks both along the nation’s eastern seaboard and inland in an arc extending from Gansu Province to Guangxi, on the southern coast. Over the past few years, the Centers for Disease Control has funded ten flu laboratories in China. The number of strains sent to the C.D.C. from China every year has now reached two hundred, up from about a dozen several years ago.
Perhaps more important, flu-watchers have a sense of when to be on the lookout for new and vicious flu strains, because any kind of major social upheaval can serve as a pandemic breeding ground. This is probably what happened with the Spanish flu: the 1918 virus was the result of a shift to h1n1. But that alone doesn’t explain its lethality. In the 1957 Asian-flu epidemic, h1n1 shifted to h2n2, and not nearly as many people died. The difference was probably the First World War.
As the Amherst College biologist Paul Ewald argues in his brilliant 1994 book, “Evolution of Infectious Diseases,” under normal circumstances the mildest offspring of any flu family will always triumph, because people who are infected with the worst strains go home and go to bed, whereas people infected with the mild strains go to work, ride the bus, and go to the movies. You’re much more likely, in other words, to catch a mild virus than a nasty virus because you’re more likely to run into someone with a mild case of flu than with a nasty case of flu. In 1918, Ewald says, these rules got inverted by the war. The Spanish flu turned nasty in the late summer in France. A mild strain of flu spreading from soldier to soldier in the trenches stayed in the trenches because none of the soldiers got so sick that they had to leave their posts. A debilitating strain, though, resulted in a soldier’s being shipped out in a crowded troop transport, then moved to an even more crowded hospital, where he had every opportunity to infect others. Wars and refugee camps and urban overcrowding give the worst flu strains a huge evolutionary advantage. If there were ever again a civil war in China, flu-watchers would be on full alert.
It doesn’t take much, however, to see that our pandemic preparedness is not foolproof. What if, for example, the new strain emerges not in the spring but in midsummer? How, under those circumstances, could a vaccine be made in time for the fall, which is when—for reasons that are unclear—any flu in temperate zones tends to strike in earnest? And what if it didn’t emerge from China, where there is good surveillance, but from Africa, say, where neither the C.D.C. nor any other W.H.O. center has the infrastructure to monitor flu strains? Most troubling, though, is that knowing a virus’s type and source doesn’t tell you nearly enough.
On May 10th of this year, for example, a three-year-old boy from Hong Kong’s New Territories came down with the flu. He died on May 21st with what looked like an unusual and severe case of viral pneumonia, compounded by Reye’s syndrome. A routine respiratory sample was taken from the boy’s body and analyzed at Hong Kong’s Queen Mary Hospital. It didn’t seem to be either h1n1 or h3n2, though, and the doctor, puzzled, forwarded the sample to the Centers for Disease Control in early July, and also to other flu labs in the Netherlands and London. “The doctor said she had a virus that was reacting differently with the reagents,” the C.D.C.’s Helen Regnery told me. “This happens sometimes, and all viruses that don’t behave well are sent here right away. But at the time the kind of reaction was such that we thought it might be a human strain. Then we got another batch from Hong Kong reacting the same way. Now it was a red flag: she’d identified two others. She E-mailed me, asking if we could confirm that particular isolate.” This was on the first Friday in August. The lab staff worked through the weekend. On Monday, Regnery got a call from researchers at the flu lab in the Netherlands. They had identified the boy’s virus. It was a pure avian flu, one that had never been seen in humans before: h5n1. “He may have had direct contact with chickens that were sick,” Regnery said. “They had chickens at his preschool. We found this out in a conference call the other night. The epidemiologists we have over there tracked down the day-care center, and they found some sick chickens.”
When I visited the C.D.C. recently, Regnery and other senior C.D.C. officials I spoke with were careful not to be alarmist when they discussed the case. The two subsequent isolates sent from Hong Kong turned out to be human flu, they told me, and none of the other children at the preschool got sick. Some members of the boy’s family had mild respiratory ailments immediately before his death, but none appeared to have caught the same flu. A C.D.C. team of three epidemiologists and a virologist recently returned from a three-week trip to Hong Kong and mainland China to help the local health authorities investigate and collect serum samples to see if anyone else was exposed, but so far nothing has come up. “For there to be a pandemic, there has to be a strain to which all or most of the population has no immunity, and that is capable of spreading from person to person,” Nancy Arden, a senior epidemiologist at the C.D.C., told me. “So far, this doesn’t meet the second criterion.”
Nonetheless, the situation was a little disturbing. Ducks fly across virtually every continent in the world, dive-bombing the landmass with flu virus. They pass it to chickens and chickens come in close contact with humans every day—on farms, in poultry markets, in chicken-processing plants. If avian flu can’t infect humans, of course, this is irrelevant. But what if the Hong Kong case means that there may now be strains of avian flu which can infect humans directly? Arden said, “There’s still a question of whether avian strains may be evolving to the point where they can replicate in humans and where a strain could be transmitted from bird to person. And, once an avian virus gets into a mammal, it’s possible that the evolution would be speeded up. No one’s so alarmed that they’re saying this is the start of the next pandemic. But it’s not something anyone would want to be complacent about.”
Then, there’s the type of flu the boy got. Avian h5 is famous among virologists as the strain that passed to domestic chickens in Pennsylvania in 1983, apparently from wild ducks. Originally, it was harmless. But as it raced from chicken to chicken in the giant commercial chicken warehouses it underwent an unusual mutation. Instead of just infecting the cells of the chicken’s intestinal tract, the virus became systemic—capable of infecting all the cells in a chicken’s body. The eyes of the chickens became swollen. The chickens had difficulty breathing. They stopped laying eggs. They became weak, and in some cases blood spots appeared in their eyes and on their legs. Upon autopsy, it turned out that they had been hemorrhaging throughout their bodies. In a matter of months, seventeen million chickens died or had to be destroyed. “It was chicken Ebola,” the flu expert Robert Webster told me. The little boy’s h5 doesn’t seem capable of the same destruction in humans. But is there any other type of h5 that would be? And, if there is, what genetic clues in the virus would tip us off? This is the big unanswered question behind our plans for the next pandemic, and it is also, of course, the big unanswered question that drives the search for the Spanish flu. What is it, specifically, that turns influenza into a killer?
To get to Longyearbyen, you fly from Oslo for about an hour and a half to Tromsø, a small town on Norway’s northern coast, and then for another ninety minutes over the Norwegian Sea to the Longyearbyen airport. The second leg of the trip retraces by air the route that the Forsete took seventy-nine years ago. It is an extraordinary journey. First, the choppy, frigid waters of the Norwegian Sea and then, out of the Arctic mist, the forbidding mountains and glaciers of Svalbard. Longyearbyen is at Svalbard’s southernmost point, huddled on the fringes of the island of Spitsbergen, a small gray stain in a blanket of white. On a clear day, from the air, it seems as if you could see the North Pole.
All this, of course, is what is so strange about the Spanish flu—that after killing so many it must now be sought out at the ends of the earth. Crosby, in the final chapter of his book on the pandemic, wonders about the disappearance of the pandemic from the American memory as well. In the Readers’ Guide to Periodical Literature, 1919-21, he reports, there are thirteen inches of column space devoted to citations of baseball stories, forty-seven inches devoted to Prohibition, twenty inches devoted to Bolshevism, and eight inches devoted to the flu. John Dos Passos, who crossed the Atlantic on a troopship on which soldiers were dying of the Spanish flu every day, has just one reference to the flu in his novel “1919” and a brief mention of the pandemic in his fictionalized war memoir, “Three Soldiers.” The pandemic is largely absent from the writing of Fitzgerald, Faulkner, and Hemingway as well, all of whom witnessed its savagery at first hand. “The average college graduate born since 1918 literally knows more about the Black Death of the fourteenth century than the World War I pandemic,” Crosby writes. He offers a number of explanations for this. In the end, though, he concludes that the virus’s figurative disappearance is of a piece with its literal disappearance, that we don’t remember it because we can’t find it. The Longyearbyen expedition is, if nothing else, an attempt to recover our memory of the Spanish flu.
Kirsty Duncan made the trip to Svalbard for the first time last spring. She had written to the governor of Svalbard seven months before, who had, in turn, approached the Norwegian medical-research community, the church in Longyearbyen, the church council, the bishop, the town council, and the victims’ families and secured approval from each. She flew to Norway in May. “I had been in Longyearbyen about a day before I went to see the minister of the church, and I was really concerned about meeting him, because of what I was asking to do,” she told me. “I introduced myself, and I said, ‘I hope in no way have I offended you or the church,’ and he said, ‘No. This is exciting, this is important work. It has to be done,’ and I was so relieved, and then he asked me ifI had been to the cemetery, and I said no, that I had no right to go there until I had spoken to him, and he said, ‘You go.’ ”
The cemetery is a ten-minute walk from the church, along a gravel road that runs parallel to the mountain. You walk away from the water and the docks, and toward the glacier, and for the entire walk the cemetery is straight ahead—a lonely stand of crosses climbing up the side of the mountain. When Duncan talked about that walk from the church to the graveyard, she looked away, her eyes misting up and her voice catching with emotion. “It was May, and everything was completely ice-covered. Completely white. Longyearbyen is in a valley, and the cemetery is up on the side of the valley floor. I knew that the seven graves I was interested in were the last seven graves at the top of the cemetery, and walking up there”—she stopped for a moment—“walking up there was really hard. I was just one year older than the oldest of them, and going to look at them made me realize that they had just come of age. You think about how they were just beginning their lives. And then you see those crosses.” ♦
Published in the print edition of the September 29, 1997, issue, with the headline “The Dead Zone.”

Malcolm Gladwell has been a staff writer for The New Yorker since 1996.
/https://public-media.si-cdn.com/filer/78/ca/78ca57a4-d760-46ae-9ff1-49a31ca0c455/uscamphospital45influenzaward.jpg)