Israel’s Uprovoked and Unanswered Attack on the USS Liberty
June 5, 2026
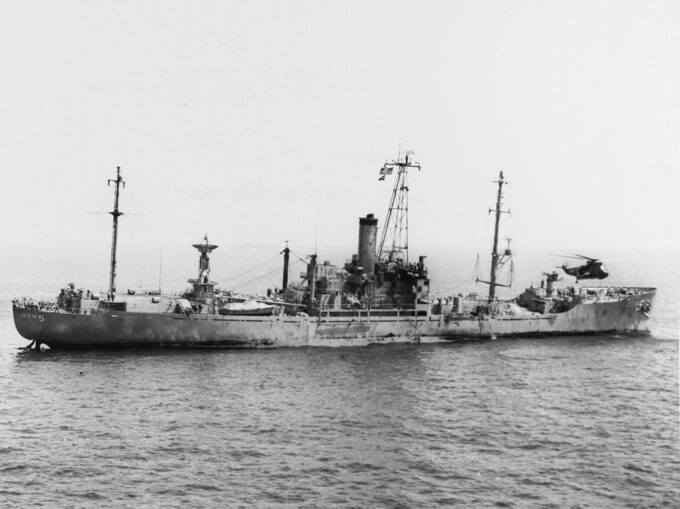
The listing USS Liberty, a day after it was attacked by Israeli gun and torpedo boats. Photo: US Navy.
In the fall of 2003, Alexander Cockburn and I were in Los Angeles for a long weekend shortly after our book, The Politics of Antisemitism, came out. Few bookstores would put it on their shelves, not even the now shuttered Midnight Special in Santa Monica, a venue where we’d both appeared several times to vibrant audiences.
We’d started our book tour with a talk in the Mission District of San Francisco, normally a safe space for the promotion of heretical opinions, where we were confronted by a group of four or five ultra-Zionist miscreants, who, in a scene out of a Marx Brothers movie, denounced us as “journalistic jihadis” and flung rotten vegetables at us, not very accurately. I recall a squishy eggplant being tossed so wildly that it splattered against a display for the Oprah Book Club. Who says there’s no Providence in this world?
A few weeks later, Bill and Kathy Christison and I were shot at as we drove back to Santa Fe following a talk outside Taos, the bullet creasing the roof of the Christisons’ car. Bill, the old CIA hand, didn’t flinch, as I cowered spinelessly in the backseat. These were tense times, with much of the country still sweating out the post-911 fever, angry, paranoid, impotent.
In LA, we had to rent our own venues, first a small art gallery in Venice and the next afternoon a coffee shop in Silver Lake. Both gigs were well-attended and went off without incident, prompting Alex to ask if I thought we might be “losing our Mojo.”
“We haven’t played Orange County, yet,” I said. “Maybe we can pick up a black cat bone and some John the Conqueror root to get our Mojo rising again before we hit Yorba Linda.”
The following evening, we met Gore Vidal at a venerable Italian eatery in old Hollywood, off Sunset Boulevard. The restaurant, Vidal explained, was just down the block from the Hacienda Arms (now called the Piazza del Sol), location of the House of Francis, the most exclusive brothel of Hollywood’s Golden Era. “Lee Francis [the madam of the establishment] put the den into iniquity,” Vidal joked. “But the real owner was MGM. The studio paid most of the bills, including bribes to the LAPD. They say Jean Harlow was sent a new girl every week and Clark Gable had his choice each afternoon in his dressing room on set. I don’t know if Madame Francis ran boys. But she must’ve. Half of Hollywood was queer. The studios liked it that way. Homosexuals were easier to control. They could be outed to the tabloids any minute, which made for fewer contract disputes.”
Vidal seemed a little forlorn to me. It had only been a few months since Howard Austen had died and he was clearly still bereft at the loss of his longtime partner and the life they shared at Ravello on the Amalfi Coast. Still, Gore dominated the conversation. Over the next two hours or so, Vidal told so many salacious anecdotes they would have filled a year’s worth of our old political gossip column, Our Little Secrets. Even Cockburn, who could hold his table talk with almost anyone, could barely pierce through Gore’s caustic monologue and eventually just tried diverting him down hilarious new avenues of vitriol and denunciation aimed at celebrities, politicians and rival writers, including the neocon transformation of the man he once declared his “dauphin,” C. Hitchens.
For most of the evening, Vidal didn’t pay much attention to me, except to say, out of the blue, that I reminded him of the young John Irving. “Not the prose, which is atrocious, but your look. Your bearing.” I didn’t see much of a resemblance; Irving was a wrestler and looked like one. I was a baseball player as a teenager and didn’t look or play quite enough like one to make it, even in the low-minor leagues. But it sounded like a compliment, so I didn’t object. Who objects to Gore Vidal anyway? “In Hollywood, everybody looks like someone else,” Vidal said with a dismissive wave of his hand. “Even the someone else you’re meant to look like.”
I cautiously reminded Vidal that all three of us had recently recorded “commentaries” for the DVD version of Tim Robbins’ film Bob Roberts. “Frankly, I didn’t watch my own or yours, but I’m sure we were all quite brilliant,” Vidal replied. “As for Tim’s excellent film, it was, I fear, quickly eclipsed by a politics that has become too absurd to satirize.”
“How so?” inquired Cockburn, who’d deftly managed to produce 45 minutes of commentary on Bob Roberts without having seen the film.
“Consider John Kerry,” Vidal quipped, in top gear now. “The senator is beginning to sound a lot like Lincoln…after the assassination.” (This is a joke that Vidal perfected over the election year, but I got the sense we may have been his first test audience.)
As the waiter uncorked the third bottle of an Italian Barolo, Alex reached into his leather satchel and handed Vidal a copy of our book, a volume Cockburn asserted was “so incendiary that we had to start our own publishing company to get it printed.” This seemed to pique Gore’s interest enough to flip through the pages of our little volume of essays on how the term “antisemitism” has been perverted and used to stigmatize and silence critics of Israel and its treatment of Palestinians.
“And you didn’t invite me to contribute?” he asked. “After all, I was a flaming anti-Semite, according to that old she-goat Abe Foxman. Imagine the puerile cast of a mind which considers that a witticism!”
“The next volume is entirely yours, Gore,” Alex offered.
As he scanned the pages, Vidal stopped about halfway through and glanced at me.
“This is you? You’re this, Jeffrey St. Clair?”
The glare was penetrating and I froze, momentarily, a little worried that I might become the object of Vidal’s withering ire, triggered by some unknown transgression against the English language.
“Yes, that’s Jeffrey, Gore,” Alex interjected. “The John Irving look-alike.” I’m not sure Alex knew who the author of The World According to Garp and The Hotel New Hampshire was (though he would have relished Setting Free the Bears), contemporary middlebrow American novelists not being at the top of his reading list.
Vidal held up our book and repeatedly jabbed an index finger at the chapter on the USS Liberty, which I had written.
“Well, Mr. St. Clair, I see you are one of the few, the very few, who have rediscovered the fate of the Liberty. I certainly hope you’ve done those men, those sailors, justice. Their country certainly didn’t. Just think of it, Israel is the only country that can attack an American naval vessel and get rewarded the next year with guns, missiles, fighter jets and money.”
A few minutes later, the waiter approached our table and said, “Mr. Vidal, your car is waiting.”
Gore rose from his seat somewhat unsteadily, squeezed my shoulder, nodded his head at Alex, grabbed his cane and hobbled out of the restaurant.
“Do you think he’ll review it now?” I asked.
“Review it? He probably won’t even remember it,” Alex snapped, scrutinizing the substantial bill we’d been left to settle.
There were no reviews forthcoming. From Gore Vidal or anyone else. Even so, The Politics of Antisemitism sold more than 10,000 copies, is still selling and, alas, will, it seems, never go out of date. Not bad for a small press with no press–only word of mouth and the CounterPunch website–behind it.
Five years later, I called Vidal to approve my edits of his introduction to A Bush and Botox World, the filmmaker and journalist Saul Landau’s book, which we were publishing that spring.
After I introduced myself, Vidal responded sharply: “You’re Mr. Liberty, right?”
I confessed I was the very same, feeling that “Mr. Liberty” was something of an improvement over being John Irving’s doppelgänger.
“Well, Jeffrey, you did fine. You did just fine. But don’t be fooled into thinking your account of this atrocity will make even the slightest difference. Mark my words. Ten or 15 years from now, we’ll be dragged deeper into the muck than we are now. We’ll be drowning in it. Faust made a better deal.”
Now, 59 years after Israel committed an unanswered act of war against the US, the US finds itself shackled to Israel in a war against Iran, a war that Trump can’t extricate himself from without the consent of Israel–a war that Israel has viciously expanded by crossing both the Litani River in Lebanon and the Yellow Line in Gaza, plunging the US deeper and deeper into the intractable muck.
Gore Vidal was right. He almost always was.
Infamy at Sea, Cover-Up in DC: Israel’s Attack on the USS Liberty

The USS Liberty being escorted to Malta after an attack by Israeli air and naval forces that killed 34 members of her crew and wounded another 171. Photo: US Navy.
In early June of 1967, at the onset of the Six-Day War, the Pentagon sent the USS Liberty from Spain into international waters off the coast of Gaza to monitor the progress of Israel’s attack on the Arab states. The Liberty was a lightly armed surveillance ship.
Only hours after the Liberty arrived, it was spotted by the Israeli military. The IDF sent out reconnaissance planes to identify the ship. They made eight trips over a period of three hours. The Liberty was flying a large US flag and was easily recognizable as an American vessel.
Soon more planes came. These were Israeli Mirage III fighters, armed with rockets and machine guns. As off-duty officers sunbathed on the deck, the fighters opened fire on the defenseless ship with rockets and machine guns.
A few minutes later a second wave of planes streaked overhead, French-built Mystere jets, which not only pelted the ship with gunfire but also with napalm bomblets, coating the deck with the flaming jelly. By now, the Liberty was on fire and dozens were wounded and killed, excluding several of the ship’s top officers.
The Liberty’s radio team tried to issue a distress call, but discovered the frequencies had been jammed by the Israeli planes with what one communications specialist called “a buzzsaw sound.” Finally, an open channel was found and the Liberty got out a message it was under attack to the USS America, the Sixth Fleet’s large aircraft carrier.
Two F-4s left the carrier to come to the Liberty’s aid. Apparently, the jets were armed only with nuclear weapons. When word reached the Pentagon, Defense Secretary Robert McNamara became irate and ordered the jets to return. “Tell the Sixth Fleet to get those aircraft back immediately,” he barked. McNamara’s injunction was reiterated in saltier terms by Admiral David L. McDonald, the chief of Naval Operations: “You get those fucking airplanes back on deck, and you get them back down.” The planes turned around. And the attack on the Liberty continued.
After the Israeli fighter jets had emptied their arsenal of rockets, three Israeli attack boats approached the Liberty. Two torpedoes were launched at the crippled ship, one tore a 40-foot wide hole in the hull, flooding the lower compartments, and killing more than a dozen American sailors.
As the Liberty listed in the choppy seas, its deck aflame, crew members dropped life rafts into the water and prepared to scuttle the ship. Given the number of wounded, this was going to be a dangerous operation. But it soon proved impossible, as the Israeli attack boats strafed the rafts with machine gun fire. No body was going to get out alive that way.
After more than two hours of unremitting assault, the Israelis finally halted their attack. One of the torpedo boats approached the Liberty. An officer asked in English over a bullhorn: “Do you need any help?”
The wounded commander of the Liberty, Lt. William McGonagle, instructed the quartermaster to respond emphatically: “Fuck you.”
The Israeli boat turned and left.
A Soviet destroyer responded before the US Navy, even though a US submarine, on a covert mission, was apparently in the area and had monitored the attack. The Soviet ship reached the Liberty six hours before the USS Davis. The captain of the Soviet ship offered his aid, but the Liberty’s conning officer refused.
Finally, 16 hours after the attack two US destroyers reached the Liberty. By that time, 34 US sailors were dead and 174 injured, many seriously. As the wounded were being evacuated, an officer with the Office of Naval Intelligence instructed the men not to talk about their ordeal with the press.
The following morning Israel launched a surprise invasion of Syria, breaching the new cease-fire agreement and seizing control of the Golan Heights.
Within three weeks, the Navy put out a 700-page report, exonerating the Israelis, claiming the attack had been accidental and that the Israelis had pulled back as soon as they realized their mistake. Defense Secretary Robert McNamara suggested the whole affair should be forgotten. “These errors do occur,” McNamara concluded.

The Israeli torpedo boats that attacked the USS Liberty.
+++
In Assault on the Liberty, a harrowing first-hand account by James Ennes Jr., McNamara’s version of events is proven to be as big a sham as his concurrent lies about Vietnam. Ennes’s book created a media storm when it was first published by Random House in 1980, including (predictably) charges that Ennes was a liar and an anti-Semite. Still, the book sold more than 40,000 copies, but was eventually allowed to go out of print. Now Ennes has published an updated version, which incorporates much new evidence that the Israeli attack was deliberate and that the US government went to extraordinary lengths to disguise the truth.
It’s a story of Israel aggression, Pentagon incompetence, official lies, and a cover-up that persists to this day. The book gains much of its power from the immediacy of Ennes’s first-hand account of the attack and the lies that followed.
Now, decades later, Ennes warns that the bloodbath on board the Liberty and its aftermath should serve as a tragic cautionary tale about the continuing ties between the US government and the government of Israel.
The Attack on the Liberty is the kind of book that makes your blood seethe. Ennes skillfully documents the life of the average sailor on one of the more peculiar vessels in the US Navy, with an attention for detail that reminds one of Dana or O’Brien. After all, the year was 1967 and most of the men on the Liberty were certainly glad to be on a non-combat ship in the middle of the Mediterranean, rather than in the Gulf of Tonkin or Mekong Delta.
But this isn’t Two Years Before the Mast. In fact, Ennes’s tour on the Liberty last only a few short weeks. He had scarcely settled into a routine before his new ship was shattered before his eyes.
Ennes joined the Liberty in May of 1967, as an Electronics Material Officer. Serving on a “spook ship”, as the Liberty was known to Navy wives, was supposed to be a sure path to career enhancement. The Liberty’s normal routine was to ply the African coast, tuning in its eavesdropping equipment on the electronic traffic in the region.
The Liberty had barely reached Africa when it received a flash message from the Joint Chiefs of Staff to sail from the Ivory Coast to the Mediterranean, where it was to re-deploy off the coast of the Sinai to monitor the Israeli attack on Egypt and the allied Arab nations.
As the war intensified, the Liberty sent a request to the fleet headquarters requesting an escort. It was denied by Admiral William Martin. The Liberty moved alone to a position in international waters about 13 miles from the shore at El Arish, then under furious siege by the IDF.
On June 6, the Joint Chiefs sent Admiral McCain, father of the senator from Arizona, an urgent message instructing him to move the Liberty out of the war zone to a position at least 100 miles off the Gaza Coast. McCain never forwarded the message to the ship.
A little after seven in the morning on June 8, Ennes entered the bridge of the Liberty to take the morning watch. Ennes was told that an hour earlier a “flying boxcar” (later identified as a twin-engine Nord 2501 Noratlas) had flown over the ship at a low level.
Ennes says he noticed that the ship’s American flag had become stained with soot and ordered a new flag run up the mast. The morning was clear and calm, with a light breeze.
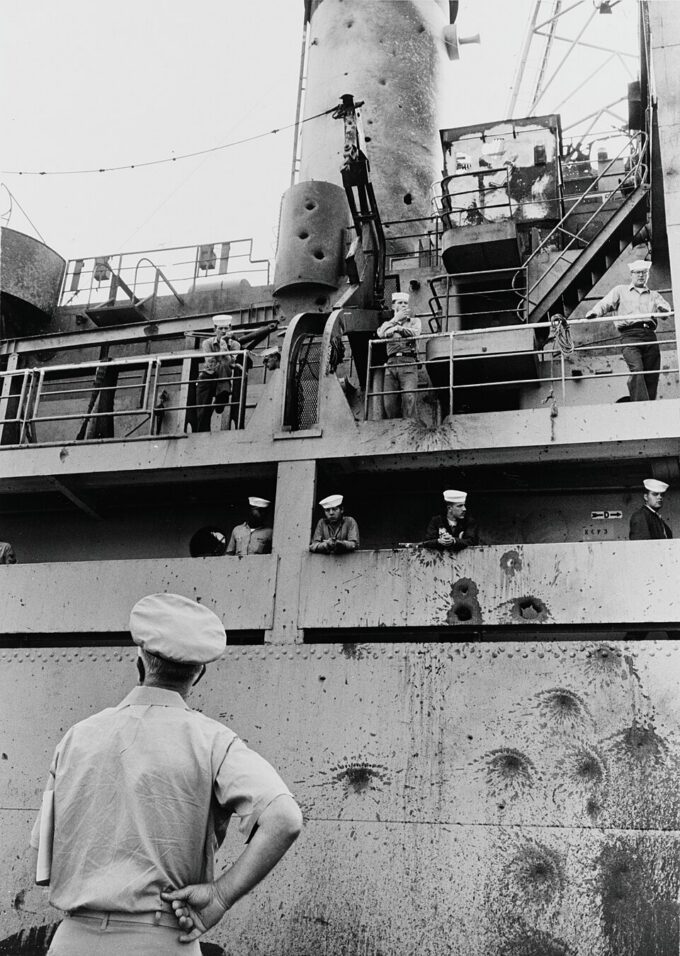
Damage to the USS Liberty from Israeli machine guns.
At 9 am, Ennes spotted another reconnaissance plane, which circled the Liberty. An hour later two Israeli fighter jets buzzed the ship. Over the next four hours, Israeli planes flew over the Liberty five more times.
When the first fighter jet struck, a little before two in the afternoon, Ennes was scanning the skies from the starboard side of the bridge, binoculars in his hands. A rocket hit the ship just below where Ennes was standing, the fragments shredded the men closest to him.
After the explosion, Ennes noticed that he was the only man left standing. But he also had been hit by more than 20 shards of shrapnel and the force of the blast had shattered his left leg. As he crawled into the pilothouse, a second fighter jet streaked above them and unleashed its payload on the hobbled Liberty.
At that point, Ennes says the crew of the Liberty had no idea who was attacking them or why. For a few moments, they suspected it might be the Soviets, after an officer mistakenly identified the fighters as MIG-15s. They knew that the Egyptian air force already had been decimated by the Israelis. The idea that the Israelis might be attacking them didn’t occur to them until one of the crew spotted a Star of David on the wing of one of the French-built Mystere jets.
Ennes was finally taken below deck to a makeshift dressing station, with other wounded men. It was hardly a safe harbor. As Ennes worried that his fractured leg might slice through his femoral artery leaving him to bleed to death, the Liberty was pummeled by rockets, machine-gun fire and an Italian-made torpedo packed with 1,000-pounds of explosive.
After the attack ended, Ennes was approached by his friend Pat O’Malley, a junior officer, who had just sent a list of killed and wounded to the Bureau of Naval Personnel. He got an immediate message back. “They said, ‘Wounded in what action? Killed in what action?’,” O’Malley told Ennes. “They said it wasn’t an ‘action,’ it was an accident. I’d like for them to come out here and see the difference between an action and an accident. Stupid bastards.”
The cover-up had begun.
+++
The Pentagon lied to the public about the attack on the Liberty from the very beginning. In a decision personally approved by the loathsome McNamara, the Pentagon denied to the press that the Liberty was an intelligence ship, referring to it instead as a Technical Research ship, as if it were little more than a military version of Jacques Cousteau’s Calypso.
The military press corps on the USS America, where most of the wounded sailors had been taken, were placed under extreme restrictions. All of the stories filed from the carrier were first routed through the Pentagon for security clearance, objectionable material was removed with barely a bleat of protest from the reporters or their publications.
Predictably, Israel’s first response was to blame the victim, a tactic that has served them so well in the Palestinian situation. First, the IDF alleged that it had asked the State Department and the Pentagon to identify any US ships in the area and was told that there were none. Then the Israeli government charged that the Liberty failed to fly its flag and didn’t respond to calls for it to identify itself. The Israelis contended that they assumed the Liberty was an Egyptian supply ship called El Quseir, which, even though it was a rusting transport ship then docked in Alexandria, the IDF said it suspected of shelling Israeli troops from the sea. Under these circumstances, the Israeli’s said they were justified in opening fire on the Liberty. The Israelis said that they halted the attack almost immediately, when they realized their mistake.
“The Liberty contributed decisively toward its identification as an enemy ship,” the IDF report concluded. This was a blatant falsehood, since the Israelis had identified the Liberty at least six hours prior to the attack on the ship.
Even though the Pentagon knew better, it gave credence to the Israeli account by saying that perhaps the Liberty’s flag had lain limp on the flagpole in a windless sea. The Pentagon also suggested that the attack might have lasted less than 20 minutes.
After the initial battery of misinformation, the Pentagon imposed a news blackout on the Liberty disaster until after the completion of a Court of Inquiry investigation.
The inquiry was headed by Rear Admiral Isaac C. Kidd. Kidd didn’t have a free hand. He’d been instructed by Vice-Admiral McCain to limit the damage to the Pentagon and to protect the reputation of Israel.
The Kidd interviewed the crew on June 14 and 15. The questioning was extremely circumscribed. According to Ennes, the  investigators “asked nothing that might be embarrassing to Israel and testimony that tended to embarrass Israel was covered with a ‘Top Secret’ label, if it was accepted at all.”
investigators “asked nothing that might be embarrassing to Israel and testimony that tended to embarrass Israel was covered with a ‘Top Secret’ label, if it was accepted at all.”
Ennes notes that even testimony by the Liberty’s communications officers about the jamming of the ship’s radios was classified as “Top Secret.” The reason? It proved that Israel knew it was attacking an American ship. “Here was strong evidence that the attack was planned in advance and that our ship’s identity was known to the attackers (for it its practically impossible to jam the radio of a stranger), but this information was hushed up and no conclusions were drawn from it,” Ennes writes.
Similarly, the Court of Inquiry deep-sixed testimony and affidavits regarding the flag-Ennes had ordered a crisp new one deployed early on the morning of the attack. The investigators buried intercepts of conversations between IDF pilots identifying the ship as flying an American flag.
It also refused to accept evidence about the IDF’s use of napalm during the attacks and choose not to hear testimony regarding the duration of the attacks and the fact that the US Navy failed to send planes to defend the ship.
“No one came to help us,” said Dr. Richard F. Kiepfer, the Liberty’s physician. “We were promised help, but no help came. The Russians arrived before our own ships did. We asked for an escort before we ever came to the war zone and we were turned down.”
None of this made its way into the 700-page Court of Inquiry report, which was completed within a couple of weeks and sent to Admiral McCain in London for review.
McCain approved the report over the objections of Captain Merlin Staring, the Navy legal officer assigned to the inquiry, who found the report to be flawed, incomplete and contrary to the evidence.
Staring sent a letter to the Judge Advocate General of the Navy disavowing himself from the report. The JAG seemed to take Staring’s objections to heart. It prepared a summary for the Chief of Naval Operations that almost completely ignored the Kidd/McCain report. Instead, it concluded:
that the Liberty was easily recognizable as an American naval vessel; that it’s flag was fully deployed and flying in a moderate breeze; that Israeli planes made at least eight reconnaissance flights at close range; the ship came under a prolonged attack from Israeli fighter jets and torpedo boats.
This succinct and largely accurate report was stamped Top Secret by Navy brass and stayed locked up for many years. But it was seen by many in the Pentagon and some in the Oval Office. But here was enough grumbling about the way the Liberty incident had been handled that LBJ summoned that old Washington fixer Clark Clifford to do damage control. It didn’t take Clifford long to come up with the official line: the Israelis simply had made a tragic mistake.

Damage to the hull of the USS Liberty from Israeli torpedoes.
It turns out that Admiral Kidd and Captain Ward Boston, the two investigating officers who prepared the original report for Admiral McCain, both believed that the Israeli attack was intentional and sustained. In other words, the IDF knew that they were striking an American spy ship and they wanted to sink it and kill as many sailors as possible. Why then did the Navy investigators produce a sham report that concluded it was an accident?
Twenty-five years later we finally found out. In June of 2002, Captain Boston told the Navy Times: “Officers follow orders.”
It gets worse. There’s plenty of evidence that US intelligence agencies learned on June 7 that Israel intended to attack the Liberty on the following day and that the strike had been personally ordered by Moshe Dayan.
As the attacks were going on, conversations between Israeli pilots were overheard by US Air Force officers in an EC121 surveillance plane overhead. The spy plane was spotted by Israeli jets, which were given orders to shoot it down. The American plane narrowly avoided the IDF missiles.
Initial reports on the incident prepared by the CIA, Office of Naval Intelligence and the National Security Agency all reached similar conclusions.
A particularly damning report compiled by a CIA informant suggests that Israeli Defense minister Moshe Dayan personally ordered the attack and wanted it to proceed until the Liberty was sunk and all on board killed. A heavily redacted version of the report was released in 1977. It reads in part:
“[The source] said that Dayan personally ordered the attack on the ship and that one of his generals adamantly opposed the action and said, ‘This is pure murder.’ One of the admirals who was present also disapproved of the action, and it was he who ordered it stopped and not Dayan.”
This amazing document generated little attention from the press and Dayan was never publicly questioned about his role in the attack.
The analyses by the intelligence agencies are collected in a 1967 investigation by the Defense Subcommittee on Appropriations. Two and half decades later that report remains classified. Why? A former committee staffer said: “So as not to embarrass Israel.”
More proof came to light from the Israeli side. A few years after Attack on the Liberty was originally published, Ennes got a call from Evan Toni, an Israeli pilot. Toni told Ennes that he had just read his book and wanted to tell him his story. Toni said that he was the pilot in the first Israeli Mirage fighter to reach the Liberty. He immediately recognized the ship to be a US Navy vessel. He radioed Israeli air command with this information and asked for instructions. Toni said he was ordered to “attack.” He refused and flew back to the air base at Ashdod. When he arrived he was summarily arrested for disobeying orders.
+++

Commander W.L. McGongile in his damaged cabin aboard the USS Liberty.
How tightly does the Israeli lobby control the Hill? For the first time in history, an attack on an America ship was not subjected to a public investigation by Congress. In 1980, Adlai Stevenson and Barry Goldwater planned to open a senate hearing into the Liberty affair. Then Jimmy Carter intervened by brokering a deal with Menachem Begin, where Israel agreed to pony up $6 million to pay for damages to the ship. A State Department press release announced the payment said, “The book is now closed on the USS Liberty.”
It certainly was the last chapter for Adlai Stevenson. He ran for governor of Illinois the following year, where his less than perfect record on Israel, and his unsettling questions about the Liberty affair, became an issue in the campaign. Big money flowed into the coffers of his Republican opponent, Big Jim Thompson, and Stevenson went down to a narrow defeat.
But the book wasn’t closed for the sailors either, of course. After a Newsweek story exposed the gist of what really happened on that day in the Mediterranean, an enraged Admiral McCain placed all the sailors under a gag order. When one sailor told an officer that he was having problems living with the cover-up, he was told: “Forget about it, that’s an order.”
The Navy went to bizarre lengths to keep the crew of the Liberty from telling what they knew. When gag orders didn’t work, they threatened sanctions. Ennes tells of the confinement and interrogation of two Liberty sailors that sounds like something right out of the CIA’s MK-Ultra program.
“In an incredible abuse of authority, military officers held two young Liberty sailors against their will in a locked and heavily guarded psychiatric ward of the base hospital,” Ennes writes. “For days these men were drugged and questioned about their recollections of the attack by a ‘therapist’ who admitted to being untrained in either psychiatry or psychology. At one point, they avoided electroshock only by bolting from the room and demanding to see the commanding officer.”
Since coming home, the veterans who have tried to tell of their ordeal have been harassed relentlessly. They’ve been branded as drunks, bigots, liars and frauds. Often, it turns out, these slurs have been leaked by the Pentagon. And, oh yeah, they’ve also been painted as anti-Semites.
In a recent column, Charley Reese describes just how mean-spirited and petty this campaign became. “When a small town in Wisconsin decided to name its library in honor of the USS Liberty crewmen, a campaign claiming it was anti-Semitic was launched,” writes Reese. “And when the town went ahead, the U.S. government ordered no Navy personnel to attend, and sent no messages. This little library was the first, and at the time the only, memorial to the men who died on the Liberty.”
+++
So why then did the Israelis attack the Liberty?
A few days before the Six Days War, Israel’s Foreign Minister Abba Eban visited Washington to inform LBJ about the forthcoming invasion. Johnson cautioned Eban that the US could not support such an attack.
It’s possible, then, that the IDF assumed that the Liberty was spying on the Israeli war plans. Possible, but not likely. Despite the official denials, as Andrew and Leslie Cockburn demonstrate in Dangerous Liaison, at the time of the Six-Day War the US and Israel had developed a warm covert relationship. So closely were the two sides working that US intelligence aid certainly helped secure Israel’s devastating and swift victory. In fact, it’s possible that the Liberty had been sent to the region to spy for the IDF.
A somewhat more likely scenario holds that Moshe Dayan wanted to keep the lid on Israel’s plan to breach the new cease-fire and invade into Syria to seize the Golan.
It has also been suggested that Dayan ordered the attack on the Liberty with the intent of pinning the blame on the Egyptians and thus swinging public and political opinion in the United States solidly behind the Israelis. Of course, for this plan to work, the Liberty had to be destroyed and its crew killed.
There’s another factor. The Liberty was positioned just off the coast of the town of El Arish. In fact, Ennes and others had used the town’s mosque tower to fix the location of the ship along the otherwise featureless desert shoreline. The IDF had seized El Arish and had used the airport there as a prisoner of war camp. On the very day the Liberty was attacked, the IDF was in the process of executing as many as 1,000 Palestinian and Egyptian POWs, a war crime that they surely wanted to conceal from prying eyes. According to Gabriel Bron, now an Israeli reporter, who witnessed part of the massacre as a soldier: “The Egyptian prisoners of war were ordered to dig pits and then army police shot them to death.”
The bigger question is why the US government would participate so enthusiastically in the cover-up of a war crime against its own sailors. Well, the Pentagon has never been slow to hide its own incompetence. And there’s plenty of that in the Liberty affair: bungled communications, refusal to provide an escort, situating the defenseless Liberty too close to a raging battle, the inability to intervene in the attack and the inexcusably long time it took to reach the battered ship and its wounded.
That’s par for the course. But something else was going on that would only come to light later. Through most of the 1960s, the US Congress had imposed a ban on the sale of arms to both Israel and Jordan. But at the time of the Liberty attack, the Pentagon (and its allies in the White House and on the Hill) was seeking to have this proscription overturned. The top brass certainly knew that any evidence of a deliberate attack on a US Navy ship by the IDF would scuttle their plans. So they hushed it up.
In January 1968, the arms embargo on Israel was lifted and the sale of American weapons began to flow. By 1971, Israel was buying $600 million of American-made weapons a year. Two years later the purchases topped $3 billion. Almost overnight, Israel had become the largest buyer of US-made arms and aircraft.
Perversely, then, the IDF’s strike on the Liberty served to weld the US and Israel together, in a kind of political and military embrace. Now, every time the IDF attacks defenseless villages in Gaza and the West Bank with F-16s and Apache helicopters, the Palestinians quite rightly see the bloody assaults as a joint operation, with the Pentagon as a hidden partner.
Thus, does the legacy of Liberty live on, one raid after another.
A version of this essay appeared in The Politics of Anti-Semitism by Alexander Cockburn and Jeffrey St. Clair.