The Ebola Crisis: The Inconvenient Truths

On Saturday, WHO Director-General Tedros Adhanom Ghebreyesus visited eastern Congo’s Bunia, a city at the heart of the Ebola outbreak, where the virus is spreading faster than the response.
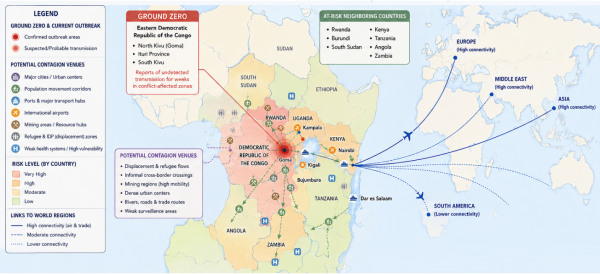
The crisis is centered in eastern Democratic Republic of the Congo (DRC), with spillovers into Uganda and rising concern across neighboring states. Official numbers remain uncertain because surveillance systems in conflict zones are incomplete.
The outbreak circulated undetected for weeks, perhaps longer, before full recognition. By the time authorities moved aggressively, transmission chains may have spread across borders, refugee corridors and informal trade networks.
Why this Ebola crisis is different
The danger does not lie primarily in the current number of cases, which remain far below the scale of COVID-19 or even the West African Ebola outbreak of 2014-16.
Historically, Ebola outbreaks have remained geographically concentrated. Although the virus is highly lethal, it is relatively difficult to transmit compared with airborne respiratory diseases.
But the present crisis is unfolding under unusually adverse conditions: war, displacement, urbanization, weak public-health systems, declining international aid capacity and growing mistrust of authorities. “Never before has an Ebola outbreak recorded so many cases so soon after its declaration,” the medical charity Médecins Sans Frontières has warned.
Eastern Congo is one of the most difficult environments in the world for epidemic control. Armed militias, population displacement and attacks on medical facilities undermine contact tracing and isolation efforts. Informal border crossings are extensive. Urban growth has accelerated faster than health infrastructure. In some affected regions, public trust in government and foreign health interventions is extremely weak.
Moreover, the current outbreak involves the Bundibugyo strain of Ebola, for which no fully established licensed vaccine exists comparable to those deployed against the Zaire strain during previous outbreaks. That sharply complicates containment.
Potential contagion links
One of the least understood aspects of the present outbreak concerns contagion linkages beyond immediate epidemiology. Let’s start with physical contagion networks: Eastern Africa’s transport corridors increasingly connect local outbreaks to regional and global mobility systems.
Cities like Kampala, Kigali and Nairobi are no longer isolated peripheral centers. They are integrated into international aviation and trade flows linking Africa to the Gulf, Europe and Asia.
Second, institutional contagion effects: Fragile health systems already weakened by debt burdens, inflation and post-pandemic exhaustion are struggling to absorb another major shock, particularly in sub-Saharan Africa.
Third, psychological and economic contagion: Financial markets, tourism flows, commodity exports and investment patterns can react violently even to limited outbreaks if fears of wider transmission intensify. The 2014-16 Ebola crisis demonstrated how panic itself can generate severe economic damage independent of the actual epidemiological scale.
Finally, geopolitical contagion: In a fragmented multipolar world, global health crises increasingly intersect with strategic competition, sanctions, debt restructuring and security concerns. Epidemics no longer operate outside geopolitics; they amplify it.
The impact of US aid withdrawal
One of the most consequential dimensions of the current Ebola crisis concerns the partial retreat of US and Western international health support over recent years.
American funding cuts and shifting priorities have weakened several pillars of global epidemic preparedness, including surveillance systems, laboratory support, emergency logistics and NGO operations across vulnerable regions. The abrupt manner these cuts have been executed has compounded the negative effects.
The broad erosion of development assistance after COVID-era fiscal strains aggravates the problem. In practice, this means slower outbreak detection, weaker field operations and reduced healthcare resilience precisely where early intervention matters most.
The retreat of preventative international health capacity is likely to ultimately increase the probability of far costlier future global emergencies.
In the case of Ebola, the Trump administration is contributing to amplified risks. Though most countries are following the WHO’s advice on travel bans, the U.S. is ignoring it.
Contagion scenarios
The first and most likely plausible scenario is a severe but regionally contained epidemic. The outbreak could produce thousands or even tens of thousands of cases regionally, while devastating local economies and healthcare systems.
In this case, intensified international response efforts eventually stabilize transmission through traditional Ebola control measures: isolation, tracing, border monitoring and behavioral adaptation. For now, this is regarded as the likeliest scenario.
The second scenario involves a wider multinational African epidemic. This becomes plausible if transmission becomes embedded along mobility corridors linking Congo, Uganda, Rwanda, Kenya, Tanzania and beyond. Refugee flows, mining routes and informal commerce networks could facilitate wider regional spread.
In this case, Ebola would remain primarily an African crisis, but one with major global economic, humanitarian and geopolitical repercussions.
The third scenario — a true global pandemic transition — remains relatively unlikely but can no longer be dismissed entirely. Sustained international spread would likely require repeated exportation into major cities combined with failures in hospital containment and perhaps viral adaptation toward easier transmission.
There is currently no evidence of such adaptation. Nevertheless, prolonged uncontrolled transmission increases evolutionary opportunities and magnifies systemic risk.
From regional emergency to global test
The present Ebola crisis has not become a global pandemic threat comparable to COVID-19. Public health officials hope it will remain regionally concentrated despite severe humanitarian consequences.
The failure to contain the Ebola crisis in its early local stage suggests that the lessons of Covid-19 pandemic have not been learned. It heralds still another tragedy of missed opportunities.
However, the world today is less institutionally cohesive, less politically cooperative and less strategically prepared for transnational crises than it was just a decade ago. Pandemic fatigue, geopolitical rivalry and fiscal retrenchment have weakened precisely the mechanisms needed for early containment.
Infectious disease containment operates according to a simple principle: outbreaks are cheapest to stop at the periphery. Once they reach major urban systems and international mobility corridors, costs rise exponentially.
It is a principle that the international community can ignore only at its own peril.
Dr. Dan Steinbock is an internationally recognized strategist of the multipolar world and the founder of Difference Group. He has served at the India, China and America Institute (USA), Shanghai Institutes for International Studies (China) and the EU Center (Singapore). For more, see https://www.differencegroup.net
No comments:
Post a Comment