It’s possible that I shall make an ass of myself. But in that case one can always get out of it with a little dialectic. I have, of course, so worded my proposition as to be right either way (K.Marx, Letter to F.Engels on the Indian Mutiny)
Friday, April 03, 2020
Hand washing a challenge for 10 million households who haven’t enough water
Many have no water at all in the home and must bring it in by hand
Health authorities say that washing one’s hands is one of the most effective ways to avoid contracting and spreading Covid-19, but the measure isn’t as simple as turning on the faucet for the one-third of Mexican households that lack daily access to water.
In Mexico, 10.5 million households do not have daily access to potable water for cleaning and drinking, and human rights experts say that this shortfall poses one of the biggest challenges to combatting the spread of the novel coronavirus.
The data published by the federal statistics agency Inegi comes as a warning after the United Nations (UN) said last week that the fight against the disease has little chance of success if people aren’t guaranteed access to clean water to wash their hands.
The data reveal that 25% of households receive water only “every now and then,” while over 7% have no access at all to water in the home and must carry or otherwise transport it from external sources.
“We were able to observe that 68% of households — 22,428,142 — receive water [consistently], while 25% — 8,411,920 — obtain it every three days, one or two times a week or every now and then,” reported the agency.
“… 7% — 2,085,208 — do not have [access to water in the home] and get it by carrying it from another home, a public tap, wells, rivers, ditches, lakes, lagoons or from tankers,” it said.
The UN’s announcement of the importance of handwashing to containing the spread of Covid-19 was accompanied by a plea to world governments to guarantee sufficient access to clean water to their most vulnerable populations.
“The fight against the pandemic has few possibilities for success if personal hygiene, the principal measure for preventing contagion, is not within reach of those who do not have access to potable water services,” said the organization.
The UN’s Human Rights Council said that limited access will make it more likely that the virus will spread among vulnerable populations with limited resources.
“Governments should apply measures to break this cycle,” said human rights specialists on the council.
The social development agency Coneval said that in Mexico, rural and indigenous communities will be the most affected by the situation.
“Indigenous communities have the least coverage within the potable water infrastructure,” said Coneval, citing different but similar data to Inegi about water access.
Amnesty International Mexico’s executive director, Tania Reneaum Panszi, told the newspaper El Universal that the pandemic is going to affect those with limited resources much differently than those of other social classes.
“Access to [water] will be one of the biggest challenges [during the pandemic]. … There are people in this country who will not be able to wash their hands. The inequality is going to be made completely visible,” she said.
She said that inequality will be seen in people whose economic situations oblige them to go to work to survive and people without access to social security and urged both the Mexican government and the private sector to take measures to protect vulnerable populations.
“It is recommended that people stay home, but this is a privilege of class. It can be done with stable working conditions, with social security and when the employer is willing,” she said.
In parts of Latin America, water shortages undermine battle with coronavirus
By Robenson Sanon and Sarah Marsh,Reuters•April 3, 2020 Outbreak of the coronavirus disease (COVID-19), in Port-au-Prince By Robenson Sanon and Sarah Marsh
PORT-AU-PRINCE/HAVANA (Reuters) - Every day, Fontus Pierre Raymond wakes up at the crack of dawn to get in line to fill buckets of water at the communal tap in his densely-packed Port-au-Prince shantytown so that his mother and seven younger siblings can wash before work and school.
Often, though, it runs dry and the 24-year-old has to trudge further to a cistern with dirtier water. So he wonders how he is supposed to follow the recommended hygiene measures to stave off the deadly new coronavirus, like frequently washing hands and social distancing.
Millions across Latin America face a similar dilemma. While underinvestment in infrastructure has long been a problem in certain parts of the region, the spread of the highly contagious disease makes poor access to water a matter of life or death.
The situation in Haiti, the poorest country in the Americas, is the most dire by far. Most homes do not receive piped water and rely instead on communal taps, water trucks or often contaminated springs.
Less than a quarter of households have basic handwashing facilities with water and soap, according to data compiled by the United Nations.
"Since they announced the pandemic (in Haiti two weeks ago), the tap has had water twice," said Mimose Pierre Raymond, 44, Fontus' mother. "But we can spend weeks without water."
Haiti has only confirmed 18 cases to date, but experts fear the COVID-19 respiratory disease caused by the virus would be more deadly there than other countries if it took hold given the widespread malnutrition and its overburdened healthcare system.
CRUMBLING INFRASTRUCTURE
Water supply coverage is, on average, better in Latin America than in Africa and Asia, according to United Nations national data, but many countries are still facing difficulties. While Haiti's water system has always been underdeveloped, that of the once-prosperous nearby Venezuela has crumbled in tandem with the economy, following years of underinvestment and widespread allegations that officials stole public funds.
Theoretically, most homes in Venezuela receive piped water. In practice, the pipes often run dry.
"We can spend months without (running) water," said Maria Dolores, a pensioner wearing a face mask and plastic gloves as she lined up to fill buckets with water from a street hydrant in a working-class neighborhood of Caracas.
In middle-class neighborhoods, many homes have tanks that store water when it sporadically comes in through the pipes. Even then, it often is not enough.
"I have a tank at home that holds 500 to 600 liters and already that's not enough when there's no running water for three weeks," said Ivan Mersly, filling up containers with water at a local cistern and carrying it home on a skateboard.
Meanwhile in Communist-run Cuba, authorities say below-average rains this year are exacerbating existing water supply problems such as leaks that cause it to lose as much as 50 percent of the water pumped from its reservoirs.
Around half a million residents are facing challenges in water supply, with Havana particularly affected, said Antonio Rodríguez, the head of the Cuban National Institute of Hydraulic Resources, last month in a televised roundtable on coronavirus prevention preparedness.
Some countries are innovating stop-gap measures to alleviate their water woes in view of the pandemic.
Cash-strapped Haitian authorities have installed some handwashing points in public squares, markets and state institutions, although many neighborhoods like Pierre Raymond's have to rely on private initiatives.
"The government is responsible but has not done one here so I did one," said community leader Ralph Apollon who has installed a tank with chlorinated water on the side of his house so his neighbors can wash their hands.
Other countries like Cuba, which has confirmed 269 cases of the new virus so far, say they are speeding up planned infrastructure projects like the installation of desalination plants. Yet locals fear that will take time.
"I'm really worried," said Jose Raul Fernandez, 46, an electrician who lives in Center Havana. "Authorities are asking us to follow hygiene measures due to the coronavirus, but without sufficient water, it's just impossible."
(Reporting by Robenson Sanon in Port-au-Prince, Sarah Marsh and Nelson Acosta in Havana, Efrain Otero and Johnny Carvajal in Caracas; Editing by Daniel Flynn, Aurora Ellis and Grant McCool)
Too much hugging, says rights group.
Human rights group slams AMLO for downplaying coronavirus danger
López Obrador's behavior sets a 'dangerous example that threatens Mexicans’ health'
The international non-governmental organization Human Rights Watch (HRW) has harshly criticized President López Obrador for putting the people of Mexico in “grave danger” with his “reckless disregard” for providing accurate information on the Covid-19 pandemic and failing to lead by example in the practice of social distancing.
HRW noted that AMLO, as the president is widely known, has “directly contradicted” the recommendations of health authorities by encouraging people to go out while officials are asking Mexicans to stay home as much as possible.
“If you can do it and you have the financial means, keep taking your family out to eat, to the restaurants, to the fondas [cheap diners] because that strengthens the family economy and the working class economy,” López Obrador said in a video posted to social media last Sunday.
HRW also criticized the president for continuing to hold rallies and attend events at which he hugs, kisses and shakes hands with supporters despite his own government’s social distancing recommendations.
While López Obrador is now heeding the advice to keep his distance from others, just a week ago he presided over a National Guard graduation ceremony in Mexico City during which he shook hands with more than 100 new guardsmen and guardswomen.
HRW also noted that when the first coronavirus case was detected in Mexico at the end of February, AMLO “blatantly misinformed the Mexican public, saying: ‘according to the information available, it is not terrible or fatal. It is not even as bad as the flu.’”
In addition, the human rights group was critical of the president’s declaration earlier this month that people should continue to hug each other because “nothing will happen.”
José Miguel Vivanco, Americas director at HRW, said that López Obrador’s behavior amid the Covid-19 crisis is “a profoundly dangerous example that threatens Mexicans’ health.”
He added that the president has “shown outrageous unwillingness to provide accurate and evidence-based information about the risks of a virus that has already killed thousands of people worldwide.”
López Obrador “needs to take this issue seriously for the sake of the health and lives of the Mexican people,” Vivanco said.
HRW noted that Mexico has some of the highest rates of obesity and diabetes in the world, meaning that Covid-19 is an even greater threat to many Mexicans.
In that context, Vivanco said that “leaders should faithfully meet their obligation to ensure people have access to accurate, evidence-based information essential to protecting their health.”
“Failure to do so is not just a violation of the right to health, but will also lead to many preventable deaths.”
Mexico News Daily Poll How would you rate the government's response to the coronavirus?
Disastrous. 57.68% (774 votes)
Not good. 27.72% (372 votes)
Not bad. 7.75% (104 votes)
Good. 6.85% (92 votes)
Total Votes: 1,342
Hospital personnel protest in México state. Hospital staff protest lack of supplies, equipment to combat virus 'We can’t go to war without rifles,' says México state pediatrician
Doctors, nurses and other hospital staff in México state protested on Monday to demand they be given the supplies they need to treat safely and effectively those infected with Covid-19, whose numbers are growing in at least a dozen municipalities in the state.
Beginning around 8:00 a.m., they gathered outside state hospitals in Toluca, Atizapán de Zaragoza, Naucalpan, Nicolás Romero, Nezahualcóyotl, Ecatepec, Tecámac, Texcoco and Ixtapaluca.
It was day two of the protest for staff of the Adolfo López Mateos state hospital in Toluca, who demanded sufficient and quality personal protection equipment after 14 nurses and one resident doctor at the facility were put into isolation and hospitalized for Covid-19.
Nurse Liliana Romero said that some supplies were sent to the hospital for the crisis, but not enough. “There aren’t any goggles or face masks. We got some body suits, but they aren’t fully sealed.”
There was a similar demonstration outside the Salvador González Herrejón state hospital, in Atizapán de Zaragoza.
“We can’t go to war without rifles,” said pediatrician Josefina Onofre Díaz. “We’re the most exposed [to the virus], those who fall first.”
Dr. Daniel Arellano of the hospital’s intensive care unit said there are not enough ventilators and other equipment to deal with the crisis.
A shipment of new beds and containers that Arellano said “we hope are full of equipment, supplies and high-grade medications” was sent to the hospital toward the end of the protest on Monday.
Elsewhere in the state, doctors, nurses and other staff from the José María Rodríguez state hospital in Ecatepec blocked a street in that city to protest a similar lack of supplies.
KEY POINTS The union representing General Electric employees is demanding the company use its full manufacturing resources to increase its ventilator output to help fill shortages caused by the coronavirus pandemic.
The members of the Industrial Division of Communication Workers of America protested Monday at the company’s aviation facility in Lynn, Massachusetts, as well as its headquarters in Boston.
The IUE-CWA said GE could leverage employees it plans to lay off to instead increase its capacity to manufacture ventilators.
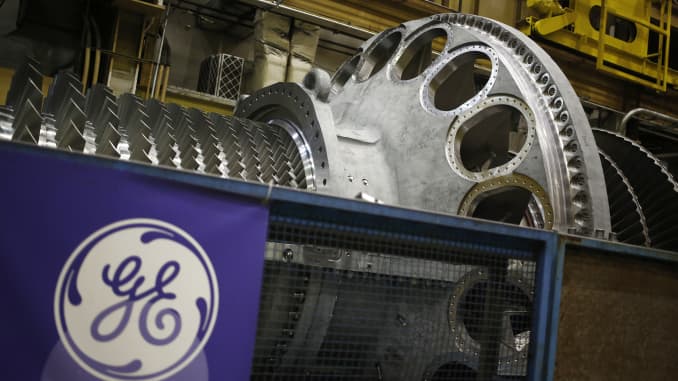
A logo is displayed next to a gas turbine at the General Electric Co. (GE) energy plant in Greenville, South Carolina, U.S., on Tuesday, Jan. 10, 2017. General Electric Co. is scheduled to release earnings figures on January 20. Sharrett / Bloomberg / Getty Images
The union representing the largest share of General Electric employees in the U.S. is demanding the company use its full manufacturing resources to increase its ventilator output to help fill shortages caused by the coronavirus pandemic.
The members of the Industrial Division of Communication Workers of America, or IUE-CWA, protested on Monday at the company’s aviation facility in Lynn, Massachusetts, as well as its headquarters in Boston after the company announced it would lay off 10% of its aviation workforce.
GE Aviation also announced that it would temporarily lay off 50% of its U.S. maintenance, repair and overhaul employees for 90 days. GE predicts these actions will save the company $500 million to $1 billion in 2020, according to a press release.
However, the IUE-CWA said that GE could leverage the employees to increase its capacity to manufacture ventilators, a piece of medical equipment that is in high demand for treating the most critical patients with COVID-19.
On Tuesday, Ford and GE Healthcare announced United Auto Workers union employees would begin manufacturing a “simplified version of GE Healthcare’s existing ventilator design” to aid patients who may experience trouble breathing caused by COVID-19.
The company said it is working “around the clock” to increase production of ventilators through its partnership with Ford.
“GE Healthcare has already doubled ventilator production capacity, with a plan to double it again by June, in addition to partnering with Ford Motor Company to further increase ventilator production. We continue to explore additional opportunities to support the fight against COVID-19, while continuing to support mission-critical work for our customers as well,” a company spokesperson said in a statement.
Union members held a silent protest standing 6 feet apart at the company’s facility in Lynn, which the company uses for its aviation manufacturing, and marched 6 feet apart at GE headquarters in Boston.
The IUE-CWA is the larger of the two unions representing GE employees in the U.S. and represents about 4,900 employees.
Correction: This story has been updated to reflect that GE announced it would lay off 10% of its aviation workforce, not its total U.S. workforce. General Electric Workers Launch Protest, Demand to Make Ventilators GE workers who normally make jet engines say their facilities are sitting idle while the country faces a dire ventilator shortage.
On Monday, General Electric factory workers launched two separate protests demanding that the company convert its jet engine factories to make ventilators. At GE's Lynn, Massachusetts aviation facility, workers held a silent protest, standing six feet apart. Union members at the company’s Boston headquarters also marched six feet apart, calling on the company to use its factories to help the country close its ventilator shortage amid the coronavirus pandemic.
These protests come just after General Electric announced it would be laying off 10 percent of its domestic aviation workforce, firing nearly 2,600 workers, along with a “temporary” layoff of 50 percent of its maintenance workers in a bid to save the company "$500 million to $1 billion.” This news came as Congress stood ready to pass a multi-trillion dollar corporate bailout that would include at least $50 billion in federal assistance and $25 billion in loans and temporary tax relief for the aviation industry, as well as a further $17 billion for federal assistance to companies deemed "crucial to national security." GE says it does not plan to request funds from the stimulus.
In a press conference, members of the Industrial Division of Communication Workers of America (IUE-CWA) explained how General Electric’s current layoffs and closures would undermine future efforts to increase ventilator production. Without experienced workers to operate now empty and idle factories, production will likely be slowed down.
IUE-CWA Local 86004 President Jake Aguanaga offered his plant, located in Arkansas City, Kansas, as an example of how much manufacturing capacity could be converted: more than 52 percent of his workforce has been laid off, and several football fields worth of factory space are currently sitting idle. “If GE trusts us to build, maintain, and test engines which go on a variety of aircraft where millions of lives are at stake, why wouldn’t they trust us to build ventilators?” he said.
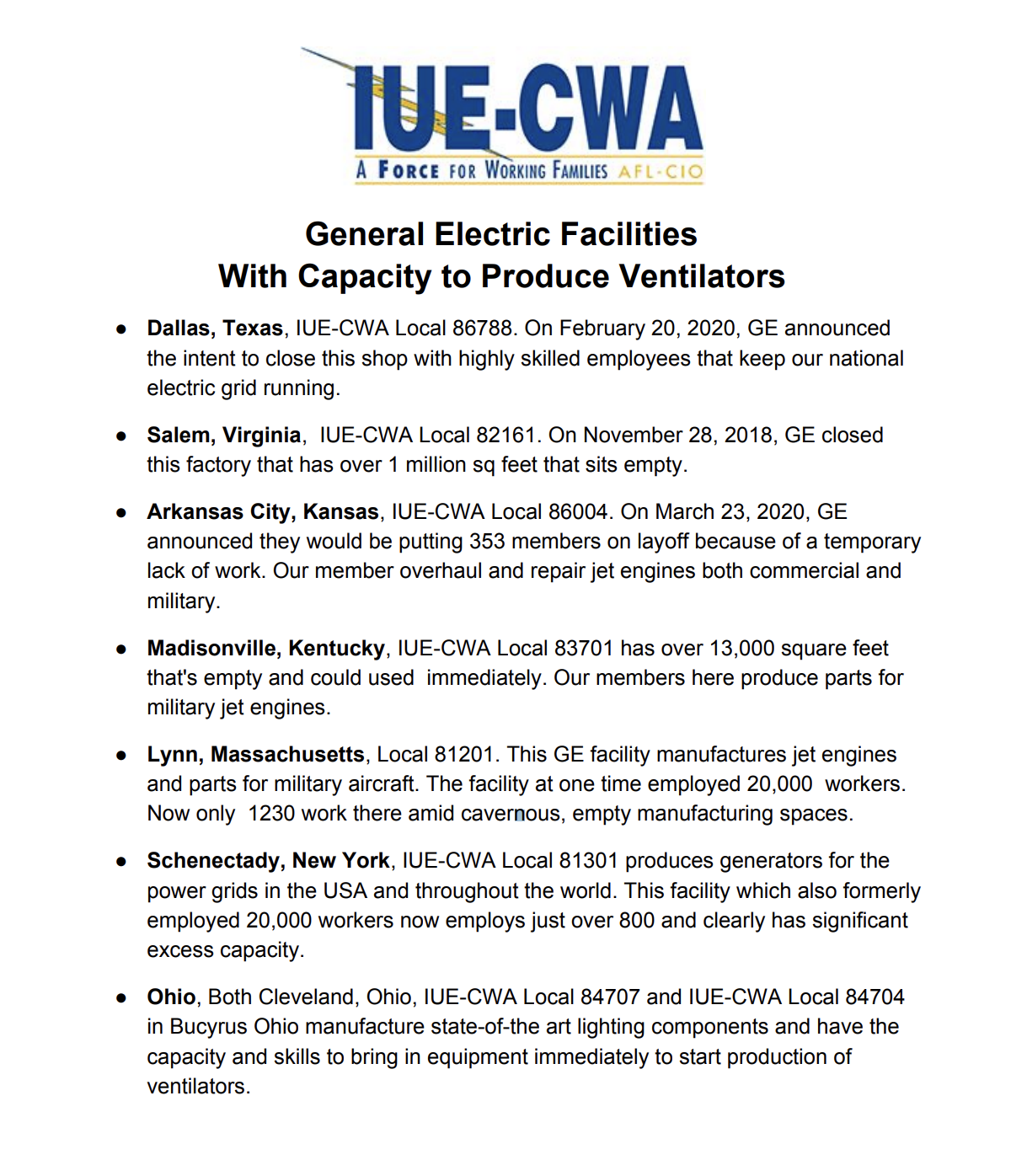
GE’s Healthcare Division is already one of the country’s largest manufacturers of ventilators, so union members believe that other factories could be converted to produce the life-saving devices. Hospitals around the country say that there is a critical shortage of ventilators, and many experts have implored President Trump to invoke the Defense Production Act to require companies to produce them. Trump finally decided to make General Motors produce ventilators over the weekend, the first in a series of deals that may eventually call on General Electric to increase ventilator supply. AN INFORMATION SHEET PUT OUT BY THE IUE-CWA
The company says it has also ramped up ventilator production in its Madison, Wisconsin factory, and said that it also needs to consider the needs of its other customers, like the U.S. military, before changing the types of products a specific factory makes.
“GE is working around the clock to increase production of much-needed medical equipment. GE Healthcare has already doubled ventilator production capacity, with a plan to double it again by June, in addition to partnering with Ford Motor Company to further increase ventilator production," the company said in a statement. "We continue to explore additional opportunities to support the fight against COVID-19, while continuing to support mission-critical work for our customers as well.”
CWA members say that they are desperate to help.
“Ventilators are desperately needed at hospitals in New York, California, Washington State, and Florida. They soon will be in short supply from the East Coast to the West Coast, from Puerto Rico to Hawaii, from Alaska and Illinois to Texas,” said CWA President Chris Shelton. “Most Americans are not aware that the best ventilators are already made by General Electric within the company’s healthcare division.”
"Our country depends on these highly skilled workers and now they’re wondering why they are facing layoffs instead of having the opportunity to use their unbelievable skills to help save lives,” said Shelton.
Update: This story's headline has been updated to clarify that the workers consider their action to be a protest and not a walkoff. It has also been updated with comment from GE.
Despite the entire world learning more about biology and immunology in the past couple of months than they ever learned in highschool, much remains unknown about Corona Virus Disease 2019, aka Covid-19, and there’s a lot of contradictory information floating around in the vacuum of that ignorance, much abetted, unfortunately, by the fecalocracy. However, an article I read this morning, about a team who tracked the course of Covid-19 infection in a bunch of ferrets, caused me to seek out the original paper, which is to be found in a journal called Cell Host & Microbe. It’s quite interesting, and I include it here:
At the bottom of the Worms & Germs page are several, uh, germane posts, notably one on Novel Corona and Wildlife Markets.
I hope this further interrogation advances your understanding of the plague, as it has mine, and I wish to thank all the good folks who brought to bear their healthy skepticism.
I’m going back to my own lab, at the corner of Corona and Lime, by way of advancing research for an Arm’s Length Negroni.
Yours in peace, biology, and social distance,
Jim
ALL WE HAVE IS EACH OTHER A Call to Action: Towards a General Strike to End the COVID-19 Crisis and Create a New World — By Cooperation Jackson March 31st, 2020 Cooperation Jackson Greetings Comrades, COVID-19 pandemic is changing the world before our very eyes. In less than 3 months, it has exposed the grotesque nature of the capitalist system to millions, ground the world economy to a halt, and revealed how truly interconnected our little planet really is. As bad as this crisis is on its own terms, it is made considerably worse by the misleadership from the White House, Congress and many state and local governments. President Trump not only failed to heed the advice of the state’s intelligence services regarding the potential threat of the coronavirus, he downplayed its severity for months, and has refused to mobilize the vast resources at the disposal of the US government to address the crisis. He continues to deny the science and proven medical advice and is now threatening to retract social distancing orders and call for everyone to return to work by the end of April. A bipartisan Congress just passed the largest corporate bailout in history, that provided paltry relief to most working people in the form of a one time payoff that won’t cover most people’s rent and utilities for a month. The Governors of Mississippi, Florida, and Georgia have refused to shut their states down and give clear stay at home orders to halt the spread of the virus. And the Federal Reserve is doing everything it can to protect Wall Street, in total disregard of the real time needs of millions of people. If Trump and his political alliies in government, Wall Street, and the corporations are successful in forcing a considerable number of workers to go back to work before the pandemic has been brought under control, it will turn into an outright calamity in the US. We cannot afford to let this happen. This is just the tip of the iceberg. Disaster capitalism and white supremacy are running amok. The Trump alliance of the neo-fascist right, combined with sectors of finance capital, the fossil fuel industry and the religious right are exploiting this crisis to accelerate climate change, reshape society and redefine the geopolitical order. In the midst of this pandemic they have eliminated critical environmental protection standards (reducing already poor air quality giving new horrible life to the Black Lives Matter slogan borne of Eric Garner’s murder, “I cant breathe” as millions struggle for air). Trump has eliminated various health and safety standards to protect workers and consumers, undermining unions and other working class organizations. He has allowed genetically modified plants to be unleashed in protected lands, expanded roundup and deportation operations, and refused to provide adequate medical treatment of federal prisoners. Brutal bipartisan sanctions on Iran and Venezuela prevent millions of poor and working class from accessing critical life saving resources, and US intervention has blocked Venezuela from receiving an IMF loan to address the COVID-19 pandemic. Right now the federal response is being driven by finance ministers and corporations, rather than the medical experts and front line workers directly addressing the response to the pandemic, abandoning the potential power of a coordinated federal response. All this is just a sample of the crimes against humanity unfolding daily at the hands of the White House. Despite the asymmetry of power between ourselves in the left and the organized working class and the forces of right, we have to do everything we can to intervene. We must stop the worst most deadly version of this pandemic from becoming a reality, and we have to ensure that we never return to the society that enabled this pandemic to emerge and have the impact it is having in the first place. We must do everything that we can to create a new, just, equitable and ecologically regenerative economy. The question is how? To fight back we have to use the greatest power we have at our disposal – our collective labor. We can shut the system down to break the power of the state and capitalist class. We must send a clear message that things cannot and will not go back to normal. In order to do this, we need to call for collective work and shopping stoppages, leading to a general strike that is centered around clear, comprehensive demands. We must make demands that will transform our broken and inequitable society, and build a new society run by and for us – the working class, poor, oppressed majority. A general strike cannot be organized through online campaigns alone, or as the result of the mere expression of a desire or even great need for a general strike. A general strike is not organized through a list of demands, though demands are necessary In order for a general strike to not only take place right now, but also be effective, we need to develop a broad united front organized around short-term and long-term aims. We need to assess connections between unions of all sorts and organized labor, and begin reaching out to other poor and working-class people from within our places of work, our places of living, our places of worship, and our places of leisure. A general strike will also take resources to sustain. We cannot count on capital to support this effort; they will attack and undermine us at every turn. So, we are going to have to call for and reply upon our collective resources. This includes our own individual purchasing power, but also the mobilization of the collective resources at the disposal of our unions, civic organizations, mutual aid, and spiritual institutions. We need to make sure that we can provide aid to workers on the frontlines of the health struggle and the frontlines of the supply chain struggles. This means providing mutual aid where warranted, as well as strike funds to support workers from losing their homes, cars, medical care, and other essential expenses. Those with the most experience in organizing strikes of all sorts – both young and old – must step up in this moment and provide general insights and strategies that can be utilized by the united front in tandem with organized labor groups that are on the same page, and these insights in addition to strategy must inform an open information campaign that not only brings attention to strike efforts, but brings in supporters from outside of our organized formations who can then employ a wide range of strategies to begin initiating mass actions without feeling isolated. The capitalists and landlords win when we are divided, fearful, and/or fighting our own battles in isolation. All it takes is enough of us breaking for them to have their way. We stand a much better chance coordinating nationally and internationally, and with organizing networks and infrastructure that are fortified with centuries’ worth of cumulative experience between the organizers who comprise them. We also stand a better chance with global attention. Those who control the land, the property, and the businesses want you to believe that this COVID-19 crisis is going to blow over soon, and that everyone will simply go back to work. They want you to believe that things will return to “normal” within a matter of months, and even weeks. Right now, poor and working-class people have an opportunity to make it clear to the ruling classes that not only was “normal” abnormal to begin with, but that we are not going to settle for a return to the social and economic conditions that created this pandemic to begin with. We should take inspiration in that we are not alone in calling for and acting upon a call for a general strike. Workers throughout the country and the world are spontaneously taking matters into their own hands. Auto workers, chicken factory workers, nurses, drivers, grocery store workers, and more are all taking independent action. Calls for a rent strike are going viral, as working poor and homeless workers are starting to occupy hundreds of vacant homes to meet their needs and practice the necessary social distancing to ensure their survival. Things are in motion and we need to build upon this momentum, quickly. This crisis changes everything. We have an opportunity to take control now, and we are ready to fight for a society in which all people can live with full autonomy without having to worry about survival. Below is the basic framing and list of preliminary demands that we think are essential to call for and act upon at this time. *General Strike! No Work, No Shopping Friday, May 1st People over Profit: Tell the Government and Wall Street that their priority must be to Save Lives, Not Profits. Returning to Work under this Pandemic is a threat to our Collective Health and Safety We Need Systems Change, Not Just Relief and Reform. The Capitalist System Can’t Resolve this Crisis. Our Demands: Protect All Frontline Workers in the Hospitals, the Supply Chains, and the Farms and Fields to ensure that they have all of the equipment and disinfectant materials that they need to keep themselves and the general public healthy Protect Asians and other vulnerable communities, including the homeless, migrants, and refugees from discrimination and attack in this time of crisis Democratize the Means of Production, Convert the Corporations and Workplaces into Cooperatives to produce what we need and distribute equitably according to need Institute Universal Health Care Now Institute Universal Basic Services Now (Education, Childcare, Elderly Care, Water, Electricity, Internet, etc.) based on Economic, Social and Cultural rights guidelines Institute Universal Basic Income Now Democratize the Finance, Credit and Insurance Industries – Bailout the People, Not the Corporations and Wall Street Decarbonize the Economy, Institute a Green New Deal based on a Just Transition, End the Fossil Fuel and Extractive Industries Now Housing is a Human Right, Decommodify Housing Now, Open all available housing stock to those who need it now Ensure there is clean drinking water for all communities, decommodify water now Cancel Our Debts, Institute a Debt Jubilee Now Close the Jails, Close the Prisons, Release the Prisoners Close the Detention Centers, Reunite the Families, Stop the Raids and Deportations Close all of the Overseas Military Bases, Cut the Military (Defense) and Spy (Surveillance) Budgets and Redirect these funds to Health Care, Social Services, Universal Basic Income and Greening Public Infrastructure and the Economy* We are calling upon all who agree with this call to join us in calling for militant action to shut the system down. This is what we are asking you to do immediately: Let us know if you agree with this call and this list of demands, or how you would add upon or strengthen them. Let us know if you would be willing to participate in a coordinating body to help organize and advance this call. This coordinating body would take on the task of building out the base of the united front, help facilitate community between its constituent parts, and facilitate the calls to action. Join us for our first zoom call on Monday, April 6th at 12 pm est/11 am cst/10 am mst/9 am pst to start building this front and advancing this call to action. To participate in the call and communicate your alignment and willingness help coordinate a broad, united front initiative email us at mayday2020generalstrike@gmail.com. Finally, this initiative is not intended to negate any of the calls already issued for a rent strike, a people’s bailout, etc. We hope to unite all who can be united, while respecting the independence of initiative of the various forces that would comprise the front. We have to apply ceaseless, unyielding pressure on the system and the forces that enable it. Let’s do so with any eye towards employing maximum unity to end this crisis and create a new world in its aftermath. Cooperation Jackson Tuesday, March 31, 2020
American Taxpayers paid millions to design a low-cost ventilator for a pandemic. Instead, the company is selling versions of it overseas.
As coronavirus sweeps the globe, there is not a single Trilogy Evo Universal ventilator — developed with government funds — in the U.S. stockpile.
Five years ago, the U.S. Department of Health and Human Services tried to plug a crucial hole in its preparations for a global pandemic, signing a $13.8 million contract with a Pennsylvania manufacturer to create a low-cost, portable, easy-to-use ventilator that could be stockpiled for emergencies.
This past September, with the design of the new Trilogy Evo Universal finally cleared by the Food and Drug Administration, HHS ordered 10,000 of the ventilators for the Strategic National Stockpile at a cost of $3,280 each.
But as the pandemic continues to spread across the globe, there is still not a single Trilogy Evo Universal in the stockpile.
Instead last summer, soon after the FDA’s approval, the Pennsylvania company that designed the device — a subsidiary of the Dutch appliance and technology giant Royal Philips N.V. — began selling two higher-priced commercial versions of the same ventilator around the world.
“We sell to whoever calls,” said a saleswoman at a small medical-supply company on Staten Island that bought 50 Trilogy Evo ventilators from Philips in early March and last week hiked its online price from $12,495 to $17,154. “We have hundreds of orders to fill. I think America didn’t take this seriously at first, and now everyone’s frantic.”
A screenshot obtained by ProPublica of a Trilogy Evo portable ventilator, sold by a medical supply company on Staten Island.
Last Friday, President Donald Trump invoked the Defense Production Act to compel General Motors to begin mass-producing another company’s ventilator under a federal contract. But neither Trump nor other senior officials made any mention of the Trilogy Evo Universal. Nor did HHS officials explain why they did not force Philips to accelerate delivery of these ventilators earlier this year, when it became clear that the virus was overwhelming medical facilities around the world.
An HHS spokeswoman told ProPublica that Philips had agreed to make the Trilogy Evo Universal ventilator “as soon as possible.” However, a Philips spokesman said the company has no plan to even begin production anytime this year.
Instead, Philips is negotiating with a White House team led by Trump’s son-in-law, Jared Kushner, to build 43,000 more complex and expensive hospital ventilators for Americans stricken by the virus.
Some experts said the nature of the current crisis — in which the federal government is scrambling to set up field hospitals in New York’s Central Park and the Jacob K. Javits Convention Center — underscores the urgent need for simpler, lower-cost ventilators. The story of the Trilogy Evo Universal, described here for the first time, also raises questions about the government’s reliance on public-private partnerships that public health officials have used to piece together important parts of their disaster safety net.
“That’s the problem of leaving any kind of disaster preparedness up to the market and market forces — it will never work,” said Dr. John Hick, an emergency medicine specialist in Minnesota who has advised HHS on pandemic preparedness since 2002. “The market is not going to give priority to a relatively no-frills but dependable ventilator that’s not expensive.”
The lack of ventilators has quickly become the most critical challenge to keeping alive many of the people most seriously sickened by the virus. Ventilators not only help people breathe but also can provide pressure that holds the lungs open so the air sacs don’t collapse.
Neither HHS nor Philips would provide a copy of their contract, citing proprietary technical information that would have to be redacted under a Freedom of Information Act request. But from public documents and interviews with current and former government officials, it appears that HHS has at times been remarkably deferential to Philips — and never more so than in the current pandemic.
From the start of its long effort to produce a low-cost, portable ventilator, the small HHS office in charge of the project, the Biomedical Advanced Research and Development Authority, or BARDA, knew that it might need to move quickly to increase production in an emergency and insisted that potential partners be able to ramp up quickly in the event of a pandemic.
But the contract HHS signed in September 2019 gave Philips almost a year before it had to produce a single Trilogy Evo Universal, and two more years to fulfill the order of 10,000 ventilators.
On the same day in July that the FDA cleared the stockpile version of the ventilator, it granted the application of Philips’ U.S. subsidiary, Respironics, to sell commercial versions of the Trilogy Evo. Philips quickly began shipping the commercial models overseas from its Murrysville, Pennsylvania, factory.
Steve Klink, the company’s Amsterdam-based spokesman, said Philips was within its rights under the HHS contract to prioritize the commercial versions of the Trilogy Evo. An HHS spokeswoman — who insisted she could not be identified by name, despite speaking for the agency — did not disagree.
“Keep in mind that companies are always free to develop other products based on technology developed in collaboration with the government,” she said in a statement to ProPublica. “This approach often reduces development costs and ensures the product the government needs is available for many years.”
Just last month, HHS gave a very different impression to Congress, hailing the Trilogy Evo it funded as a breakthrough in its campaign for pandemic preparedness.
“This game-changing device, considered a pipedream just a few years ago, is now available at affordable prices to improve stockpiling and deployment” in an emergency, the agency told Congress in a budget document delivered on Feb 10.
But less than two weeks later, officials overseeing the Strategic National Stockpile approached Philips with an urgent appeal: Start making our ventilators. On March 10, Philips agreed to a modification of the HHS contract — one that called for the company to produce the Trilogy Evo Universal “as soon as possible,” a spokesperson said.
However, in a subsequent statement, the HHS spokeswoman said Philips is only required to deliver the ventilators “as they are completed.” Klink, the company spokesman, said Philips was only committed to meeting the original contract deadline of 10,000 ventilators by September 2022.
Had government officials insisted that Philips first produce the ventilators that taxpayers paid to design, the government could conceivably be distributing all 10,000 to hospitals now. Last year, Philips plants in Pennsylvania and California produced 500 ventilators of various models per week; they sped up to 1,000 per week earlier this year, Klink said. At that pace, the stockpile ventilators could have been completed even if Philips devoted only part of its lines to their production.
Klink said the reason the company is not producing the stockpile ventilator is because it has not yet been mass-produced and would require time-consuming trial runs. In the current crisis, it’s faster and more efficient to continue producing the versions it is already making, he said.
Asked if Philips could hand over its Trilogy Evo Universal design to another manufacturer, he argued that the fundamental constraint on production is not the company’s assembly lines but its dependence on more than 100 smaller companies around the world that make the 650 parts needed for a hospital ventilator.
“We cannot sell a ventilator with only 649 parts,” he said. “It needs to be the whole 650.”
It is difficult to assess how much profit motives might be driving Philips’ decisions about which ventilators to produce because the company does not disclose how much it charges different clients for commercial models.
Jeff Marshall, a senior marketing manager at Philips Respironics, demonstrates the commercial version of the Trilogy Evo in a HomeCare Magazine video filmed last year. (Obtained by ProPublica via YouTube)
The commercial version of the Trilogy Evo has had its own problems. Not long after it began selling the ventilators last summer, Philips sent out recall notices to customers in Europe and the U.S., alerting them to a software glitch that prompted the devices to shut down without sounding their alarm. The software has since been updated and the problem solved, the company said.
Klink said Philips hopes to be making 4,000 ventilators of all types each week in the U.S. by October, and that it would prioritize “those communities and countries that need it the most.”
But as the pandemic spreads, desperate global demand for the commercial models of the Trilogy Evo is driving up prices sharply, and evidence from the chaotic open market for the devices raises questions about Philips’ stated commitment to prioritize the neediest.
On Staten Island, a saleswoman at No Insurance Medical Supplies, who would give her name only as Jeanette, said the company was selling to “anyone who calls,” including doctors and individuals. The company’s first shipment of 50 devices sold out quickly, but an additional five ventilators arrived on Friday. The company requested 148 more, but Philips Respironics said it could only provide 11 ventilators by April 6, she said. The company’s prices are determined by what the manufacturer charges, she said.
The competition abroad is also intense. On March 12, the regional government of Madrid, one of the cities hardest hit by the virus, bought 10 Trilogy Evo ventilators from a Spanish medical supply company for about $11,000 each. In Budapest, Hungary, the Uzsoki Street Hospital announced that a local property development company had donated two “ultra-modern” Philips Trilogy Evo ventilators on March 18.
The struggle has grown so fierce that last week, a trade group representing ventilator manufacturers asked the head of the Federal Emergency Management Agency to decide for the manufacturers whom they should sell to first.
“We would appreciate the Administration’s leadership and the advice of clinical and other experts within the Administration in deciding how to allocate these products in the most effective way,” the Advanced Medical Technology Association wrote in a letter to FEMA Administrator Peter Gaynor.
Medical experts and public health officials have believed for nearly two decades that they needed a less-expensive and simpler-to-operate portable ventilator that could be made and distributed quickly in an emergency.
“This is not a new problem,” said W. Craig Vanderwagen, a former senior HHS official who oversaw studies that led to the government’s early efforts to design and build a low-cost portable ventilator for such eventualities. “We knew back in the 2000s that ventilators were going to be critical in pandemic preparedness. That was a clear gap that we identified.”
In the early 2000s, American public health experts and government officials were gripped by a sense of urgency they had not felt before. The 9/11 attacks and the anthrax scare that followed underscored the need for sweeping new actions to keep the country safe. Outbreaks of Avian influenza — first reported in Hong Kong in 1997 — exposed the public health system’s vulnerability to new, highly fatal pathogens from overseas. The George W. Bush administration’s disastrously slow and inept response to Hurricane Katrina in 2005 prompted widespread calls for the government to strengthen its ability to deal with a growing array of emergencies, from new, highly contagious diseases to previously unthinkable terrorist attacks.
One obvious vulnerability was to a viral pandemic or a chemical or biological attack that would ravage the lungs of its victims, setting off a cascade of cases of what doctors call Acute Respiratory Distress Syndrome, or ARDS.
“None of us expected an event on the scale of what we’re going through now,” said Dr. Lewis Rubinson, a pulmonologist who participated in several of the early government-sponsored medical studies. “We had to guess: What would the patients look like? What we predicted correctly was that we could face massive cases of ARDS.”
By the early 2000s, officials at the Centers for Disease Control and Prevention had already begun working to stockpile a few thousand ventilators for such an eventuality, former officials said. But studies by medical experts and government scientists — including sophisticated models of what might occur in the event of various disasters, outbreaks or attacks — suggested a bigger problem. Hospitals could be crippled not only by shortages of complex and costly ventilators, but also by a lack of the trained respiratory technicians who are generally required to operate the machines.
The experts envisioned one important solution: a portable ventilator that was less complex than hospital machines and could be more quickly produced, safely stockpiled and widely distributed in emergencies. They envisioned a device that could be deployed in field hospitals like the ones that authorities are now rushing to create in Central Park and elsewhere.
Volunteers set up a field hospital in New York’s Central Park on Monday. Portable ventilators, like the Trilogy Evo Universal, would have been especially useful for field hospitals, medical experts said. (Bryan R. Smith/AFP via Getty Images)
The job of bringing such a device to life fell to BARDA, an innovative office of HHS that was established in 2006 to help the country prepare for pandemic influenza, new types of infectious diseases or an attack or accident involving chemical, biological or radiological weapons.
Much of BARDA’s work has been focused on developing potentially critical vaccines and other medicines that are not necessarily profitable for big pharmaceutical companies. The agency often works with medical researchers at the National Institutes of Health and elsewhere, identifying promising therapies and other innovations, and then forms partnerships with private biotechnology or other companies to create the drugs and move them through various stages of regulation.
In 2008, BARDA began trying to find a company that could make a ventilator that would be inexpensive — ideally, less than $2,000 each — and could be simple enough to use that “inexperienced health care providers with limited or no respiratory support training” could operate the devices during a pandemic, according to the agency’s solicitation for bids.
BARDA also anticipated the shortage of parts and competing priorities that the ventilator industry now faces. Companies bidding for the contract had to show they could secure the parts needed to “ramp up production to supply at least” 1,700 ventilators per month and 10,000 in six months’ time. The companies also had to pledge that government “contracts will be honored during a pandemic,” the initial solicitation said.
With only a couple of bids, BARDA settled on a small, privately held ventilator company in Costa Mesa, California, Newport Medical Instruments Inc. BARDA and Newport signed a $6.4 million contract in September 2010, specifying that the money would be doled out incrementally as the company met various milestones.
But in May 2012, Newport was purchased by a larger Irish medical device company, Covidien, for $108 million. Covidien quickly downsized and asked Rick Crawford, Newport’s former head of research and development and the lead designer of the BARDA ventilator, to finish up the project without any staff assigned to him. Crawford said he took a job with another company.
“I don’t know how you finish a project when nobody reports to you,” he recalled thinking.
A former BARDA official who worked on the project said that Covidien began raising issue after issue and demanded more money. BARDA agreed, eventually tacking on almost $2 million more to the price tag, records show. Even so, Covidien abandoned the project.
A spokesman for the still-larger firm that acquired Covidien in 2015, Medtronic, said that the prototype ventilator created by Newport Medical “would not have been able to meet the specifications required by the government, nor at the price required.” In a statement responding to a story in The New York Times, Medtronic said it left the federal government with all the designs and equipment created in the project.
Several former BARDA officials said such outcomes come with their territory. Like big pharmaceutical companies, they had to take chances, especially in the development of vaccines.
“There are going to be risks like that when you partner with businesses,” said one former senior BARDA official, who, like others, asked for anonymity because she was not authorized to speak for the agency. “It’s a problem that we at BARDA had encountered before, where a company changed hands and changed priorities.”
In March 2016, less than two years after signing its ventilator contract with BARDA, Philips Respironics agreed to pay $34.8 million to settle a Justice Department lawsuit under the False Claims Act and the Anti-Kickback Statute. Justice lawyers accused the manufacturer of effectively paying kickbacks to medical suppliers to buy its masks for sleep apnea. The company also agreed to abide by a five-year Corporate Integrity Agreement with HHS inspector general that imposed a series of oversight measures on the company’s operations.
With BARDA’s continuing support, Philips finally won FDA approval for the Trilogy Evo Universal ventilator in July 2019. Klink, the Philips spokesman, said the $13.8 million from HHS covered only a portion of the design and development costs for the ventilator and that the company invested more.
Rubinson, now the chief medical officer of Morristown Medical Center in Morristown, New Jersey, praised the BARDA effort as essential, adding that if 10,000 ventilators seems like a small number in the COVID-19 crisis, it had to be understood in the context of government officials’ typical unwillingness to buy equipment it might only need in an emergency.
“They could have bought a million ventilators,” he said. “And then you would be writing about the boondoggle of all these devices that never got used.”
Today, the government’s failure to obtain the Trilogy Evo Universal is seen by some experts as the real game changer.
“Even if a few months ago we had taken dramatic action to develop these kinds of ventilators, it would have been better,” said Hick, the emergency medicine specialist in Minnesota. “If I had a ventilator that cost $4,000 rather than $16,000, I’d be in better shape. We can buy a lot more of them.”