The harmful behaviors of profit-driven healthcare companies—from tax dodging to insurance denials to carelessness with patient safety—stem from the same illness: a disregard for the community they serve.
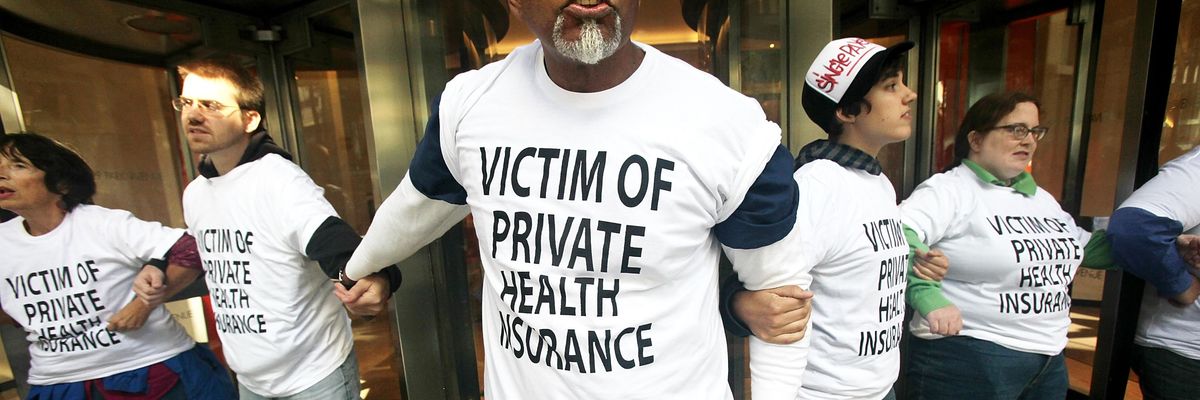
Healthcare reform supporters participate in a sit-in inside the lobby of a building where Aetna insurance offices are located September 29, 2009 in New York City.
(Photo by Mario Tama/Getty Images)
William Rice
Nov 02, 2025
Even though most of us think of healthcare as a human right, the reality is that in the United States the provision of healthcare is big business. It places profits over people, demonstrating that priority through tax dodging, price gouging, insurance denials, and unsafe conditions for patients, as documented in a recent joint report from our two organizations, Americans for Tax Fairness and Community Catalyst.
The report, “Sick Profits,” highlights how seven healthcare corporations have together saved over $34 billion in federal taxes thanks to the 2017 Trump-GOP tax law recently extended by the current Trump administration and Republican Congress. They paid for those corporate tax breaks in part by cutting Medicaid and jeopardizing health coverage for 15 million people, and failing to preserve the enhanced premium tax credits for people buying health insurance through the Affordable Care Act (ACA) Marketplaces.
RECOMMENDED...
75% of US Voters Are Concerned About Surging Healthcare Premiums

‘No Question’ More People Will End Up With Fake Insurance If ACA Subsidies Expire: Expert
We currently have public policy that cuts taxes on corporations while ignoring nearly two-thirds of people who believe that big companies are not paying enough. Instead, healthcare corporations have each enjoyed hundreds of millions—in most cases, billions—of dollars in tax savings thanks to the Republican tax law, the most expensive part of which was a two-fifths cut in the corporate tax rate. They have also saved taxes by exploiting loopholes that the law (and its extension) failed to close, including in the accounting for stock options and the treatment of profits shifted offshore.
Not surprisingly, the companies examined in the report did not use their tax savings to lower prices, hire more providers, or improve patient care. No, the money went instead to higher executive compensation and increased payouts to shareholders through dividends and stock buybacks.
We must demand more transparency, fairer tax policy, and better oversight of these institutions.
Additionally, companies are maximizing their profits by simply not paying for care. By demanding “preauthorization” for a dizzying number of procedures then routinely denying approval, insurers can save billions at the expense of their policyholders. High percentages of initial denials are overturned on appeal, showing that “no” is simply the initial default position, taken in the hopes that patients and doctors won’t push the issue. Claim denials often result in medical debt and can also disrupt treatment for chronic medical conditions, delay or deny access to lifesaving care, and lead to avoidable complications—or even death.
Claim denials affect the health and well-being of people every day. They are people like Little John Cupp, who began feeling short of breath and experienced swelling in his feet and ankles. His doctor recommended a catheter exam to determine whether the arteries in his heart were blocked. However, the medical benefits management company EviCore (owned by Cigna) twice denied the catheter exam while eventually approving a much lower-cost stress test. The delay in diagnosis proved catastrophic. Less than two days after Mr. Cupp received the stress test, he died of cardiac arrest.
The tragedy of the end of Mr. Cupp’s life demonstrates the incredibly real risks that the first obstacle to getting care creates. Unfortunately, clearing that hurdle and receiving approval for care does not ensure quality. You could find yourself getting treatment at a facility saving money for shareholders by reducing staff and failing to maintain safe and hygienic conditions. NBC News aired a six-part investigation of hospital-operator HCA Holdings that uncovered, in the words of our report, “roaches in the operating room, leaking ceilings, essentially unmonitored vital signs, overworked nurses, overcrowded emergency rooms, closed departments, and other threats to patient health and safety.”
Or you may receive care at a facility owned or controlled by private equity interests. One cautionary tale is Prospect Medical Holdings, which operated hospitals and other health facilities in multiple states and was driven into bankruptcy after it was acquired by a private equity firm that extracted over $650 million in debt-financed dividends from the targeted company. While the private equity partners enjoyed lucrative payouts, patients suffered from unsanitary conditions, supply shortages, insufficient staffing, and shuttered departments.
Our diagnosis is simple but serious. The harmful behaviors of profit-driven healthcare companies—from tax dodging to insurance denials to carelessness with patient safety—stem from the same illness: a disregard for the community they serve. We must demand more transparency, fairer tax policy, and better oversight of these institutions. That means closing tax loopholes, raising the corporate tax rate, curbing the routine denials of coverage, and strengthening regulatory oversight of health facilities. That’s the only way to ensure that people’s needs are prioritized over corporate profits.
Remote patient monitoring boosts primary care revenue and care capacity
Remote physiologic monitoring (RPM)—digital tools that track patients’ health data between visits—shows promise for improving chronic disease management and reshaping primary care delivery, according to a new study at Columbia University Mailman School of Public Health. While prior studies have examined how RPM affects patients who use the technology, this is the first study to quantify the impact of RPM on practices, including its effects on practice revenue, care delivery, and resource allocation across patients. The findings are published online in the journal Health Affairs.
“RPM services are often touted as a way for practices to both improve patient care and increase revenue, but it’s not a given that this will happen.” said study author Mitchell Tang, PhD, assistant professor of Health Policy and Management at Columbia Mailman School of Public Health.
Using national Medicare data, the researchers identified 754 primary care practices that began billing for RPM between 2019 and 2021. The researchers found that primary care practices adopting RPM saw a 20 percent increase in Medicare revenue in the next two years compared with similar practices that did not adopt RPM. Most of the increase stemmed from RPM billing, although roughly one-quarter came from added care management and outpatient visits.
Most surprisingly, according to Tang and his co-authors, adopting practices did not reduce access for patients not receiving RPM. “There was concern that the added time and resources to provide RPM to some patients would come at a cost – other patients in the practice might struggle to get care,” said Tang. On the contrary, practices saw more patients overall, with much of the added activity focused on individuals with higher disease burdens—many of whom were non-White or dually eligible for Medicare and Medicaid.
“In a time when many call for a strengthening of primary care, our study offers cautious optimism that technologies like RPM can make primary care more accessible, proactive, and patient-centered,” said co-author Ariel D. Stern, PhD, professor of Digital Health, Economics and Policy at the Hasso Plattner Institute, University of Potsdam. However, the authors caution that unchecked widespread adoption could substantially increase Medicare spending. “Thoughtful reimbursement policies, such as evidence-based limits on monitoring duration and patient eligibility, are key to incentivize high value RPM services and ensure sustainability of RPM moving forward.”
Other co-authors are Felippe Marcondes, Massachusetts General Hospital; and Ateev Mehrotra, Brown University.
The study was supported by the Commonwealth Fund.
Columbia University Mailman School of Public Health
Founded in 1922, the Columbia University Mailman School of Public Health pursues an agenda of research, education, and service to address the critical and complex public health issues affecting New Yorkers, the nation and the world. The Columbia Mailman School is the third largest recipient of NIH grants among schools of public health. Its nearly 300 multi-disciplinary faculty members work in more than 100 countries around the world, addressing such issues as preventing infectious and chronic diseases, environmental health, maternal and child health, health policy, climate change and health, and public health preparedness. It is a leader in public health education with more than 1,300 graduate students from 55 nations pursuing a variety of master’s and doctoral degree programs. The Columbia Mailman School is also home to numerous world-renowned research centers, including ICAP and the Center for Infection and Immunity. For more information, please visit www.mailman.columbia.edu.
Journal
Health Affairs
Article Title
Practices That Adopted Remote Physiologic Monitoring Increased Medicare Revenue And Outpatient Visits
.jpg)